Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
The 99th Health Economics Study Group (HESG) meeting has just taken place (5-7th January 2022) at the University of Leeds. The HESG always makes for a great conference with excellent discussion and input into ongoing research. This is partly down to the unique set up of the meeting, whereby authors submit their work but they do not give a presentation of it. Instead, a discussant is assigned to read their paper and present a discussion of the research, forming a discussion agenda to encourage the audience to engage and input their thoughts and ideas.
The format truly allows for spontaneous brainstorming among the delegates and more often than not the authors leave with lots of interesting ideas, comments and suggestions to take forward in improving their work.
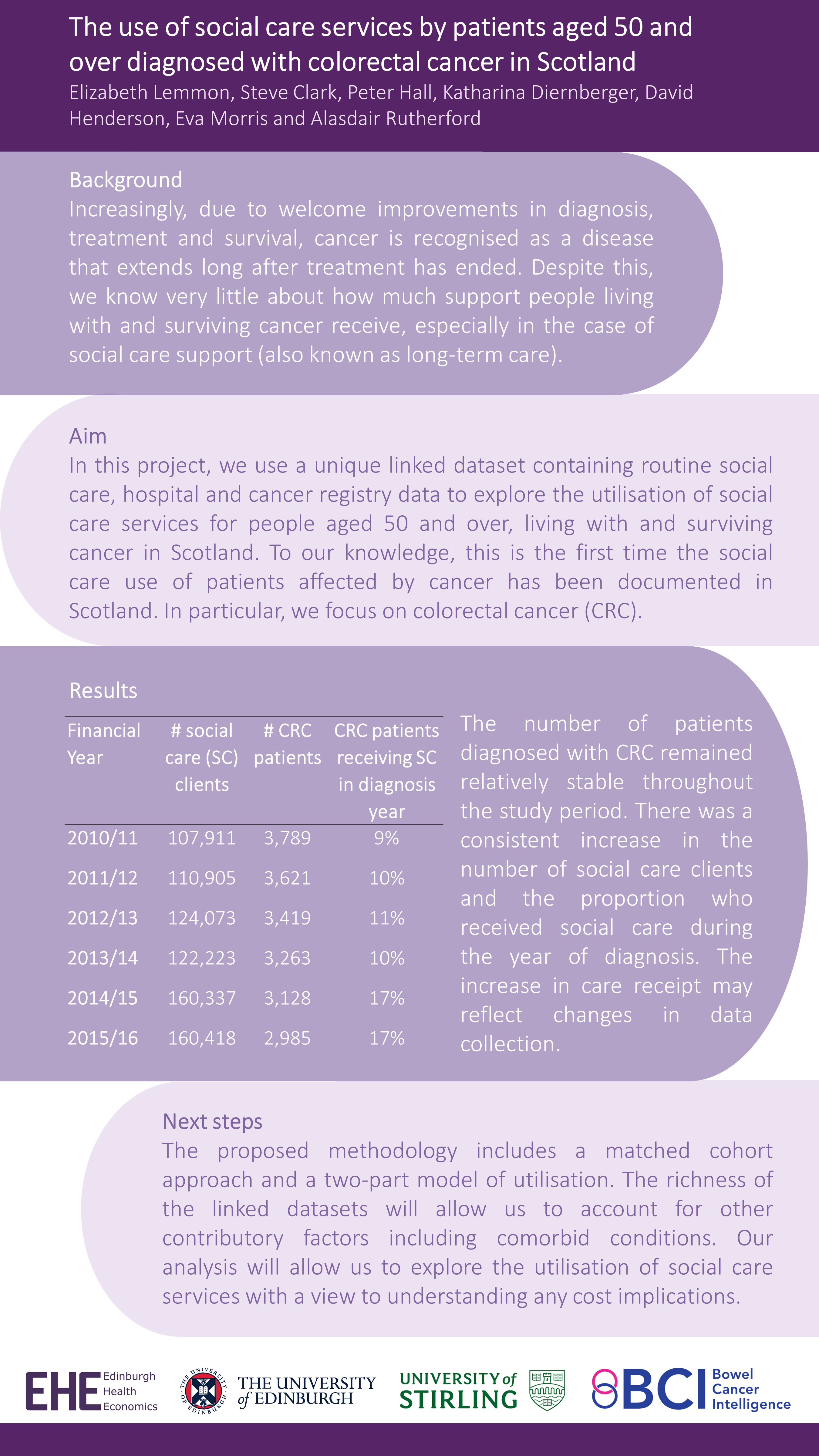
This Winter we were delighted to have our own Research Fellow, Giovanni Tramonti, representing Edinburgh Health Economics at the meeting. Giovanni was a discussant for a paper and kindly presented Elizabeth Lemmon’s et al’s work in the poster session – “The use of social care services by patients aged 50 and over diagnosed with colorectal cancer in Scotland”.
This work is the first in Scotland to analyse national data on social care service use by patients diagnosed with colorectal cancer. Check out the full poster below (all results are preliminary):
For any queries please contact Lesley Innes (she@abdn.ac.uk)
SHE was launched in 2019 to support, promote and further develop health economics in Scotland. SHE is a collaboration of health economists from Scotland’s Universities, NHS and Government. Our aim is to bring together researchers and users of health economics to explore the development and application of health economics in Scotland.
The PRC is a European Research Centre consisting of 17 international and 8 national collaborating centres. They plan and conduct international multicentre studies within palliative care, focusing on pain, cachexia and health care services. On the 30th January, the TVT (Two Versus Three Step) study, primarily run by the centre in Edinburgh, presented the initial clinical and health economics results at the PRC Seminar in Oslo ahead of the main results being published.
The TVT Study “An international, multicentre, open randomised parallel group trial comparing a two-step approach for cancer pain relief with the standard three-step approach of the WHO analgesic ladder in patients with cancer pain requiring step two analgesia” recruited patients in the UK, Mexico, Uganda and Israel and was comparing the 3-step approach for pain control currently recommended by the WHO* to a 2-step approach omitting weak opioids.
The primary outcome was time to achieving stable pain control, where stable pain control was defined as the first day of three consecutive days with average pain score ≤3 on a numeric rating scale of 0-10. The trial also looked at a potential increase in opioid-related side effects.
This was a very interesting trial from a health economic viewpoint, taking into account the different costing systems within the participating countries. Though the quality of life component (EQ-5D-5L) was captured in all countries, a full economic evaluation was only possible for the UK as the country specific value set was readily available.
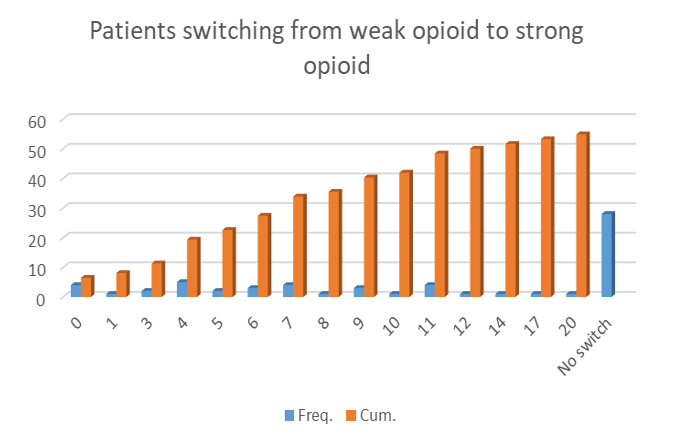
The main results of the study can be summed up fairly quickly – omitting step 2 (weak opioids) showed no significant difference in terms of pain control, lead to a reduction in opioid related side effects, is cheaper and patients -reported better outcomes for quality of life. Further to this, more than half of the patients who started on a weak opioid had to switch to a strong opioid in order to achieve pain control. The link to the full publication will be added as soon as the results are published.
Figure 1: Preliminary results from the TVT study. Number of Patients who needed to switch from a weak to a strong opioid within 20 days.
The introduction of the presentation highlighted the importance of health economics within palliative care (as a main tool for decision making within the health care sector) and tried to clarify misconceptions about health economics. It focussed on the challenges we are facing in terms of collecting costs, measure patients’ quality of life and putting a value on “life improvements” in this particular setting. This part of the presentation facilitated interesting discussion at the conference and some ideas for possible future collaborations.
After the seminar I stayed in Oslo for the weekend to catch up with friends and use the opportunity to visit the Henie Onstad Art Centre in Oslo which is currently hosting the “Picasso 347” (below), and “Claude Monet and Bærum” exhibitions as well as “Yayoi Kusamas’ – Hymn of Life” (at the top of this post). I can highly recommend a visit!
*WHO 3-step-approach:
Step 1. Non-opioids (non-steroidal anti-inflammatory drugs [NSAIDS], acetylsalicylic acid [ASA, aspirin] and paracetamol [acetaminophen]) for mild pain.
Step 2. Add an opioid for mild to moderate pain (Codeine, Tramadol).
Step 3. Add opioid for moderate to severe pain (morphine) titrated to pain relief or alternatively to occurrence of dose-limiting adverse events (AE).
The National Cancer Research Institute Annual Meeting in Glasgow 2019 marked an important milestone for members of the ECTU health economics group involved in the Lothian Cancer Data Intelligence Project (LCDI). It marked the end of an 18 month collaborative project to explore the completeness, data quality and scope of a comprehensive linked cancer regional dataset accessed by NHS Lothian Analytical Service. The project, partially funded by the Association of the British Pharmaceutical Industry, Pfizer UK, Novartis Pharmaceuticals UK Ltd, AstraZeneca UK and NHS Lothian and funded through Joint Working with Roche Products Ltd, also sought to explore the need for real world data and how to facilitate data requests from different stakeholder groups.
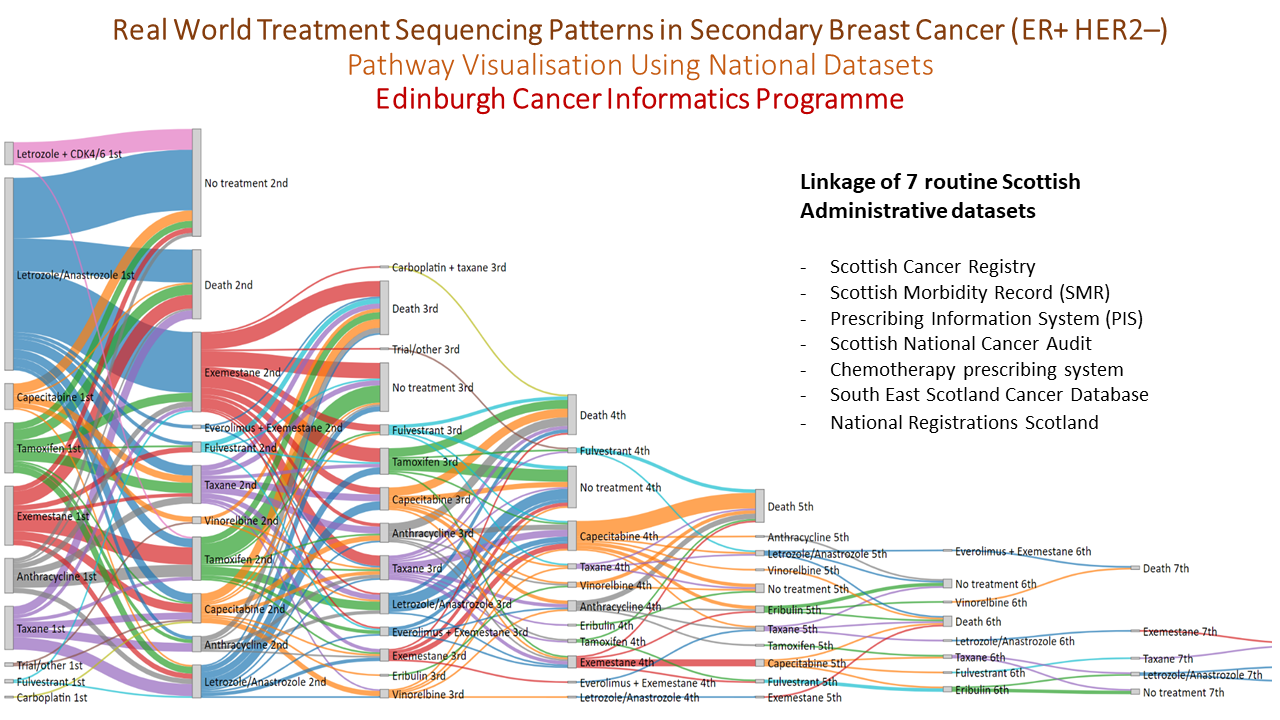
In a final meeting the key deliverables of the study were presented: a data dictionary and data quality report in the form of a wiki within the public domain and a research governance framework managed by NHS Lothian ready to pilot data requests. An important part of the project was a series of worked examples, modelled around a relevant research question, which was used to test out the processes and instructions developed as part of the LCDI study. The largest of these research questions was pathway visualisation (featured below) using national datasets to look at treatment sequencing patterns in secondary breast cancer (ER +ve HER2 –ve). This was developed into an abstract and presented at the NCRI 2019 meeting by Dr Ashley Horne as part of the Silent Theatre!
Learning from the LCDI project has led to the launch of the ‘Edinburgh Real World Data Service’ which is run jointly by the Lothian Research Safe Haven Team and the Edinburgh Cancer Informatics Programme with the objective of improving the availability and use of real NHS data to inform new reimbursement models that can ultimately provide better value medicines for NHS patients.
Learn more about the Edinburgh Real World Data Service here.
Health Economics at the 9th International Seminar of the European Palliative Care Research Centre
At the end of October (23rd to 25th), I travelled to Krems in Austria to attend the 9th International Seminar of the European Palliative Care Research Centre (EPCRC). In this post, I will offer my thoughts on the conference and tell you a little about my work which I presented there.
This was the second time I have attended the EPCRC conference- last year it was held here in Edinburgh. Whilst I enjoyed the conference last year, my reflection was that the health economics voice was definitely lacking. So, I was really hoping for good things for the conference in Krems- especially since for me this meant travelling to my home turf! I am happy to report that I was not disappointed. This year’s presentations included a lot of health economic considerations and health economics featured as a core topic throughout. For example, a talk by Professor Nathan Cherny form Israel was mainly focussed on the Health Technology Assessment process and how it links to the Magnitude of the Clinical Benefit scale. Anna Kitta from Austria and David Blum from Switzerland presented study proposals in the area of eHealth mentioning the potential costs savings for the health care systems through to technological innovation.
I also had the great opportunity to present on the Friday morning of the conference. Having attended the conference before, I knew that the audience won’t come from a health economics background. I was therefore mindful that the mention of economics alongside end of life care might have triggered in their minds the ever present myth that Economists want to take resources away from these settings. I therefore made it my mission to ensure that I convinced the audience otherwise! I decided to split my presentation into two parts. I started with the topic “The (in)compatibility of health economics and end of life care”. In this first part, I introduced some of the key health economics ideas and summed up the importance and the challenges that health economics faces, particularly with respect to end of life care. I also outlined the current situation in the UK and presented some new developments in methodological research. Hoping that I had managed to bust some health economics myths, the second part of my presentation covered the “Health economics in the EPAT study”. In this part, I showed a bit of applied health economics, presenting the economic results of a cluster randomised controlled trial testing a systematic approach in the assessment and management of cancer pain. Both presentations were well received and prompted lively discussions, so I was very happy with that.
The overall quality of the presentations at the conference, as well as the presented topics, were very well chosen and incredibly relevant to the developing field of health economics within end of life care. I got the impression that early palliative care is a major focus within the community and there is definitely a shift towards making palliative care services more flexible and patient centred. Another commonly discussed topic, which linked well with my presentation, was the potential “overtreatment” of patients in the last phase of their life.
An additional main focus of the conference was on Patient Reported Outcome Measures (PROMs) , which is of great importance for the methods development of health economics. I could take away that not just the health economists but also clinical professionals are very aware that patient questionnaires designed for a curative setting are not fit for purpose in an end of life situation.
I hope to attend next year’s conference and I am curious to see if the trend of increasing awareness and representation of health economics continues. You’ll see below some photos from the lovely Austrian dinner which the conference organisers put on for us, with traditional music and dances performed by the children group from the “Wachauer Trachten und Heimatverein Krems”.
It’s been just over one month since the official launch of Scottish Health Economics (SHE) at Discovery Point in Dundee. Set up by the Health Economics Research Unit (HERU) in Aberdeen (find out more about SHE here), “SHE seeks to act as a vehicle for widening engagement with health economics in Scotland, bringing together users and producers of health economics who are interested in the development and application of health economics in Scotland. All activities will draw on the extensive experience and expertise Scotland offers in health economics” (SHE Terms of Reference, 2018).
Since the launch of SHE on the 3rd of October, we’ve had time to reflect and it’s safe to say we are more excited than ever about the future for health economics research in Scotland! In this post, we reflect on the event and highlight some of the take home messages.
Overview of the day
The tone for the day was set by Mandy Ryan, Director of HERU, who gave an enthusiastic welcome to all SHE participants. From this point onwards, the health economics energy in the room was palpable!
Next up, Rachel Baker, Professor of Health Economics at Glasgow Caledonian University, provided an overview of health economics research in Scotland. Of noticeable interest was the useful maps she had prepared, pin pointing where us health economists, both within academic and governmental institutions, are hiding. Although Stirling was left out of the picture (Seda Erdem and colleagues quick off the mark to rectify that!), the map surprised everyone in the room as to the sheer numbers of health economists and other bodies contributing to health economics research going on in Scotland.
Following Rachel’s introduction, Marjon van der Pol, Deputy Director of HERU, talked about capacity building in health economics, and strategies for attracting the next generation of health economists.
The rest of the day was packed with excellent presentations (and a delicious lunch) from academics across the SHE community on a number of interesting health economics research questions, with reflections from the policy community including the Scottish Government, Healthcare Improvement Scotland, NHS Education Scotland and NHS Health Scotland. The academic presentations included our own Research Assistant, Alistair Bullen, who gave an elevator presentation on the use of PACE Statements as source of qualitative secondary data to inform attribute selection in discrete choice experiments.
Whilst all of these presentations were extremely interesting and really showcased the wealth of health economics research going on in Scotland, perhaps the most constructive part of the day was the afternoon breakout sessions (where I think we all agreed we could have spent all day!). The sessions allowed for the opportunity to discuss what we want to get out of SHE, including activities, training, funding opportunities, and the possibility of an annual meeting.
Prof Cam Donaldson summed up the day perfectly in his closing remarks, commenting on the unmistakable enthusiasm that charged the room throughout the event.
Take home messages
As a group, we believe that the SHE network offers a starting point for collaborations with other health economics researchers in Scotland that we can build on going forward. Simply knowing and being aware of the research going on in Scotland is in itself useful to identify who holds expertise in a particular area. At the same time, SHE will allow links to form between academic researchers and the policy community, ensuring that Scottish health economics research is contributing in the issues that matter most to the people of Scotland.
Overall, we felt that the take home message from the day was really the unique position that Scotland is in and the potential that exists for collaborative work between and across academic institutions and government.
We recently completed the SHE event survey so we will wait to see the outcome of that and very much look forward to seeing how SHE develops and contributing to the networking potential that SHE offers.
EHE would like to thank all of the organisers and presenters who made the day worthwhile!
Health Economics Study Group and Discrete Choice Experiments
I am the primary researcher on INFO-BC. We plan to implement a discrete choice experiment (DCE). A DCE is a type of stated preference exercise where respondents make decisions hypothetical scenarios. Our team identified opportunity to use DCE’s in a secondary breast cancer setting. At the start of July I attended the Summer Health Economics Study Group (HESG) at the University of East Anglia (UEA), needless to say one of my main objectives was to discover what my peers in other parts of the UK doing in the area of preference elicitation. I found the three studies particularly interesting and have provided a summary of each of them here:
Moffatt. P, King. M, Viney. R, White. B, Butler. L, 2019. Impact and detection of straightlining response in health surveys (working paper)
The problem of straightlining is prominent in DCEs. Straightlining is when a respondent does not engage in a DCE and is instead found to be consistently choosing at random or choosing according to arbitrary factors, such as always choosing the option on the left. The authors demonstrated the problem of straightlining in an example DCE. They also propose methods to identify straightliners and mitigate the problem. The proportion of straigliners identified was high at 45.2%, although there were concerns from the audience that the DCE used in the study was particularly complex and was therefore likely to have a higher proportion of straighliners. The methods which excluded individuals identified as straightliners appeared to provide more reliable estimates, although it remains to be seen if the same method would have the same results in the case of a more typical DCE design where there is likely to be a smaller proportion of straightliners.
McNamara. S, Tsuchiya, A. Holmes, J, 2019. Which preferences? choice architecture and normative health economics (working paper)
Stated preference exercises all have a choice architecture which affects how respondents interpret information and the decisions they make. This in turn impacts the resulting preferences. In health economics the results of stated preference can have real world effects on the decisions to provide or not provide treatments and technologies. In this study the authors illustrate how choice architecture can affect preferences using the example of a stated preference exercise eliciting public aversion to health inequalities. The authors address three key questions.
If preferences are architecture sensitive, should we be using them in health-economic evaluation?
If preferences are to be used in this way, what type of preference should we be using?
How should we be structuring choice architectural decisions?
In summary the authors argue for the use of preferences assuming the approach is reasonable. They propose four questions to help Heath Economists structure their choice architecture. Finally they call for closer collaboration of Health Economists, behavioural scientists, philosophers, and policy makers to address the issue the sensitivity of preferences for choice architecture.
Boyers. D, Van der pol. M, Watson. V, 2019. The impact of ex-ante correction methods on hypothetical bias in Discrete Choice Experiment responses: A case study in dental care (working paper)
I acted as the discussant for this paper. The authors experimented with methods designed to mitigate hypothetical bias from their DCE. Hypothetical bias specifically refers to bias that arises when respondents fail to respond to a DCE in the same way that they would respond in an equivalent real life scenario. There was some evidence that two interventions went a small part of the way to mitigate hypothetical bias, these interventions were an honesty oath and a consequentiality script. To simplify the interventions: the honesty oath asked respondents to tick a box before the experiment and thereby promise to give honest responses; the consequentiality script informed respondents of the consequences the DCE is likely to have on policy decisions. The honesty oath was accompanied with the added complication that the completion rate was 10.3% lower than the baseline. The general verdict of the myself audience was that this is an interesting area for further research but that one would have reservations about implementing the proposed interventions unless stronger evidence was produced.








 The tone for the day was set by
The tone for the day was set by 

