Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
The 99th Health Economics Study Group (HESG) meeting has just taken place (5-7th January 2022) at the University of Leeds. The HESG always makes for a great conference with excellent discussion and input into ongoing research. This is partly down to the unique set up of the meeting, whereby authors submit their work but they do not give a presentation of it. Instead, a discussant is assigned to read their paper and present a discussion of the research, forming a discussion agenda to encourage the audience to engage and input their thoughts and ideas.
The format truly allows for spontaneous brainstorming among the delegates and more often than not the authors leave with lots of interesting ideas, comments and suggestions to take forward in improving their work.
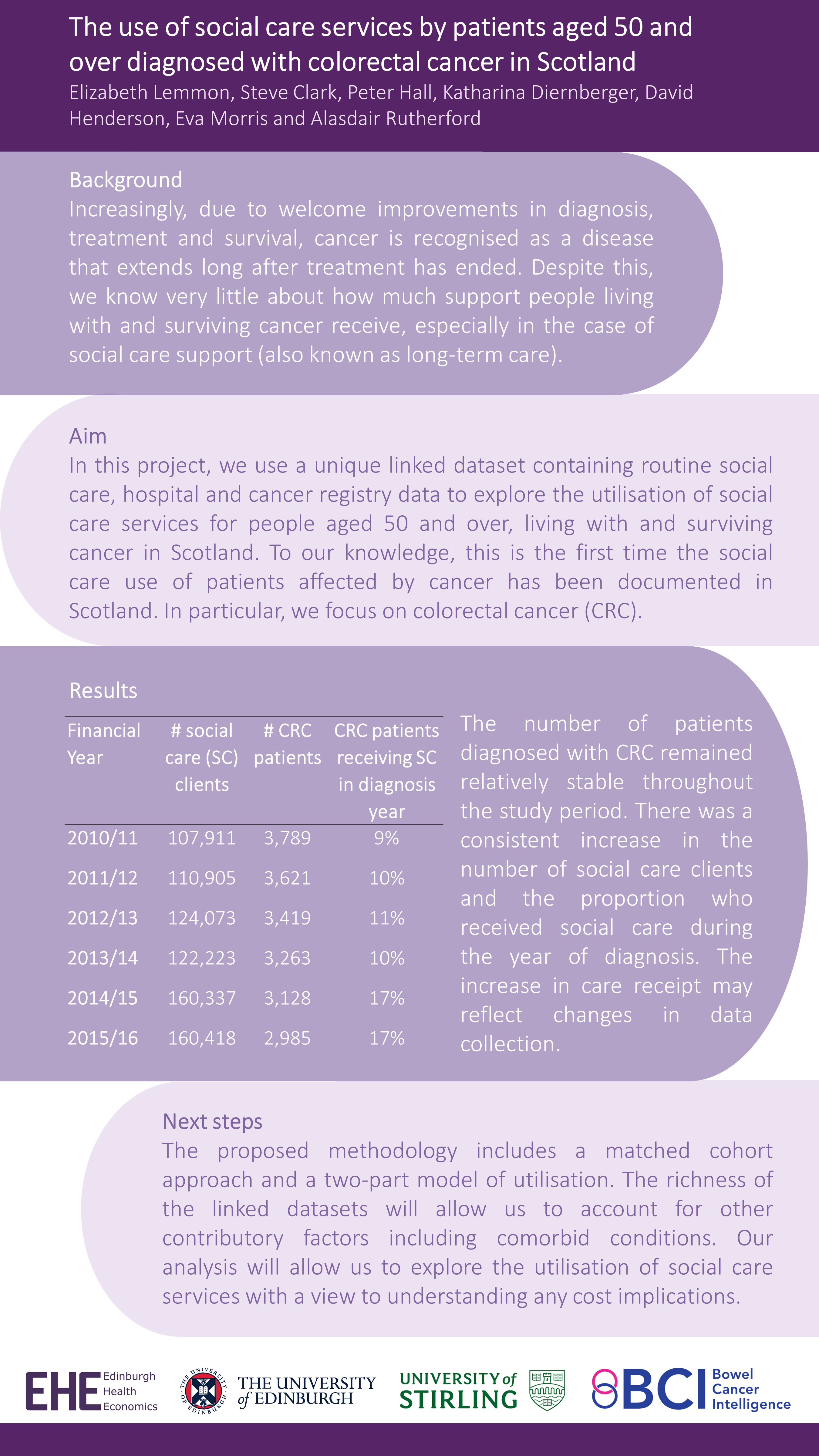
This Winter we were delighted to have our own Research Fellow, Giovanni Tramonti, representing Edinburgh Health Economics at the meeting. Giovanni was a discussant for a paper and kindly presented Elizabeth Lemmon’s et al’s work in the poster session – “The use of social care services by patients aged 50 and over diagnosed with colorectal cancer in Scotland”.
This work is the first in Scotland to analyse national data on social care service use by patients diagnosed with colorectal cancer. Check out the full poster below (all results are preliminary):
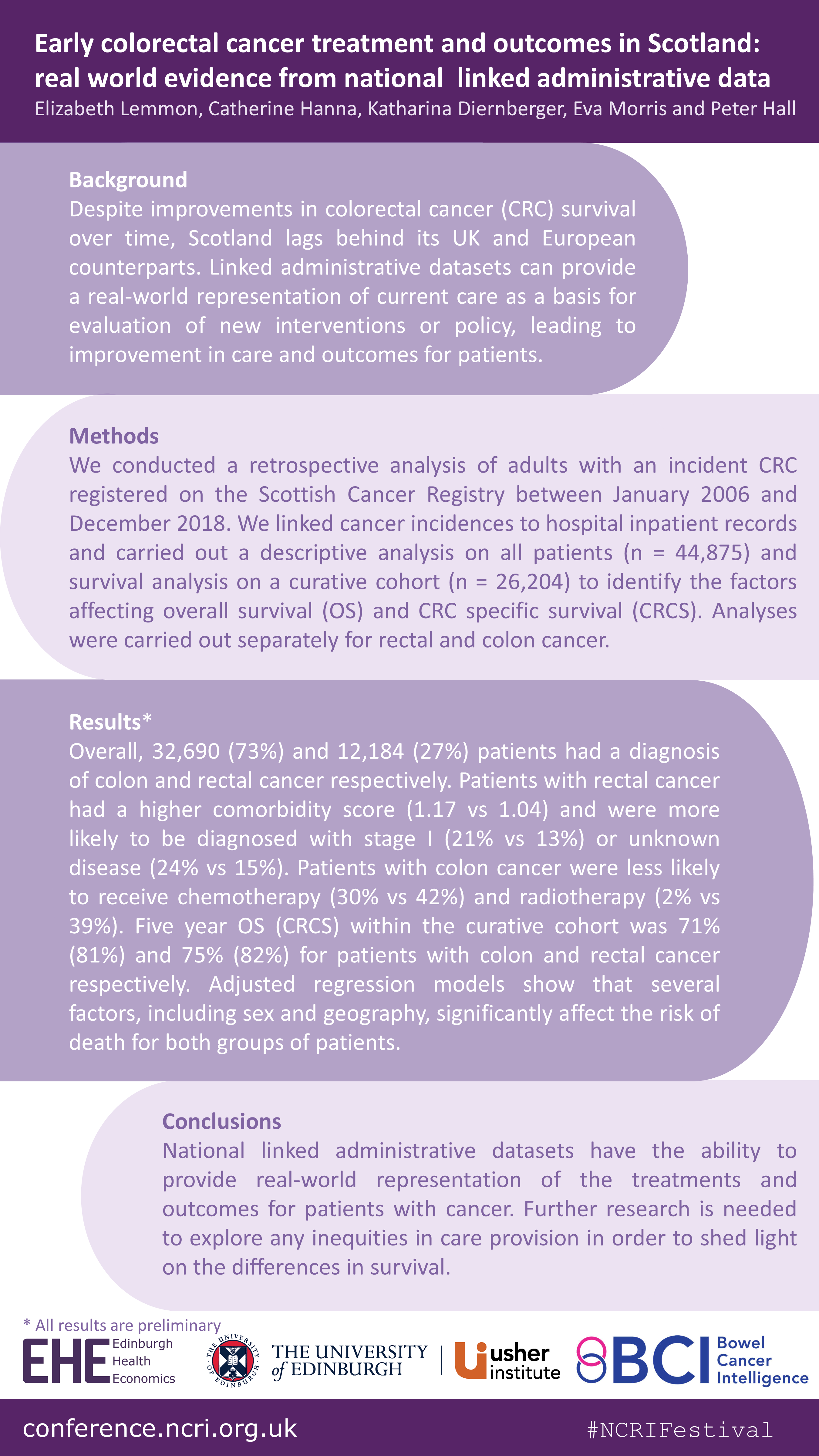
Last month (8-12 November), the Scottish Bowel Cancer Intelligence UK team at Edinburgh Health Economics attended the National Cancer Research Institute (NCRI) Festival: Making cancer research better together, with a poster on their recent work “Early colorectal cancer treatment and outcomes in Scotland: real world evidence from national linked administrative data”.
You can see more plain language summaries for the wider Bowel Cancer Intelligence programme on the BCIUK website.
Background: Whenever a patient interacts with the healthcare system, data is routinely collected, this is called “Administrative Healthcare Data”. This data can be used to provide information on screening, surveillance, existing health conditions, diagnosis, treatments and patient outcomes. It can also be used to provide information on the real-world cost of healthcare. The data is held in individual datasets, which can be linked together to provide more information than just one dataset alone.
In the UK, Administrative Healthcare Datasets are generally held separately within each nation. In Scotland, cancer data is collected by the cancer registry. This dataset contains a lot of information such as the date of diagnosis and the type and stage of cancer, but it does not include detailed information on the treatment that was delivered. In order to be able to see a full picture of what the cancer services currently look like, the cancer registry data needs to be linked to other Administrative Healthcare Datasets.
The aim of this project is to create a linked dataset to allow mapping of the bowel cancer landscape in Scotland to identify differences in the treatment offered to patients and the outcomes associated with the different treatment approaches. An additional aim is to calculate the healthcare resource needed for bowel cancer diagnosis and treatment on a national scale, and the cost of providing this.
This manuscript documents the process of creating a specific and complete bowel cancer dataset for research in Scotland.
What we did: There were four main stages in accessing and linking datasets on a national level.
Stage 1 – The first stage in accessing the data was to define the study requirements to apply to the Public Benefit and Privacy Panel (PBPP) for Health and Social Care in Scotland. The role of the PBPP is to weigh up the public benefits of granting access to healthcare data against the risks that the sharing of the data poses to an individual’s privacy.
Stage 2 – The second stage was to acquire the datasets to transfer them into the National Safe Haven (NSH). The NSH is a secure platform where the data can be used for research and analysis.
Stage 3 – All datasets that were to be released to the research team to analyse were checked by the electronic Data Research and Innovation Service (eDRIS) to make sure they matched the approved specification. The linkage of the datasets was performed by eDRIS once all the pre-checks had been completed.
Stage 4 – After the data linkages had been performed, the datasets were transferred to the National Safe Haven where researchers, with the correct approvals, could access the data. In this setting, all patient information like names and addresses were removed.
Conclusion: Linked Administrative Healthcare Datasets have huge potential to aid understanding of how patients interact with healthcare services and provide a detailed picture of the care they receive. This project demonstrates that the creation of a national linked administrative dataset is possible, by using bowel cancer data in Scotland as an example. It is however only possible through substantial effort and collaboration between researchers and the central team coordinating the data transfers and linkages.
The linked datasets have huge potential public and patient benefit by enabling researchers to analyse real world cancer data to improve outcomes for patients as well as the delivery of cancer services.
Several forces are contributing to an increase in the number of people living with and surviving colorectal cancer (CRC). However, due to the lack of available data, little is known about the implications of these forces. In recent years, the use of administrative data to inform research has been increasing. Administrative data is collected routinely ‘by government departments and other organisations for the purposes of registration, transaction and record keeping, usually during the delivery of a service’ (Woollard, 2014). Examples include hospital admissions data, education records and tax records.
The aim of one of our recent pieces of work was to investigate the potential contribution that this type of data could have on the health economic research of CRC. To achieve this aim, we conducted a systematic review of the health economic CRC literature published in the United Kingdom and Europe within the last decade (2009– 2019).
Our specific objectives were:
To summarise the existing health economic research of CRC in the UK and Europe;
To identify whether and what types of administrative data were used within this research;
To explore the benefits and limitations of using administrative data in this research;
To discuss the ways in which administrative data, using Scotland as an exemplar, could contribute to this research in the future
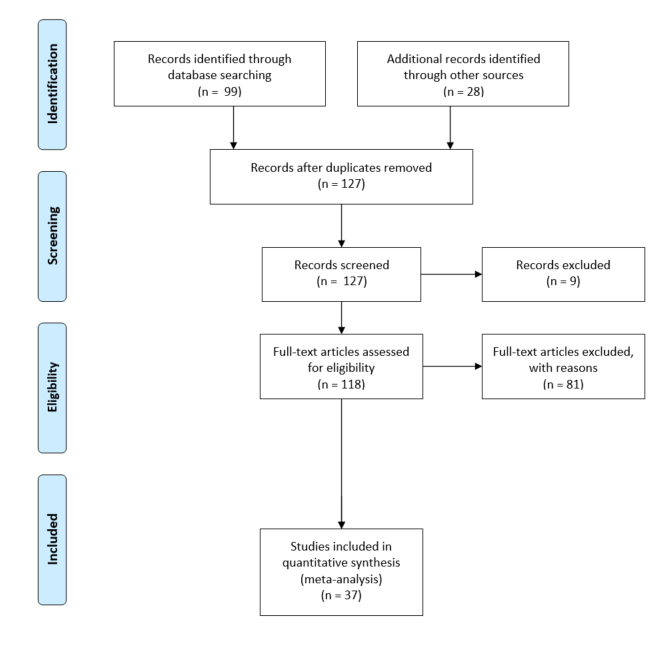
The literature search identified thirty- seven relevant studies, which we divided into economic evaluations, cost of illness studies and cost consequence analyses.
Findings:
We found that the use of administrative data, including cancer registry, screening and hospital records, within the health economic research of CRC is commonplace. However, we found that this data often come from regional databases, which reduces the generalisability of results.
Further, we found that administrative data appear less able to contribute towards understanding the wider and indirect costs associated with the disease, particularly with respect to social care and indirect costs such as unpaid care.
We also found that very few papers adopted a societal perspective when carrying out their evaluation meaning that often only direct medical care costs were included.
Finally, we found that administrative data were less able to contribute when it comes to measuring patient health related quality of life (HRQoL) and preferences for those health states, which is vital particularly in EEs.
We explore several ways in which various sources of administrative data could enhance future research in this area. If you want to find out more, head on over to the European Journal of Cancer Care website where you can read the article in full.
For the past two years, Edinburgh Health Economics have offered an options module in Health Economics to undergraduate 3rd and 4th year economics students at Edinburgh (ECNM10082). The module, led by Dr Elizabeth Lemmon with Aileen Neilson as co-lecturer and Alistair Bullen as Tutor, aims to provide students with an introduction to the key concepts, methods and understanding of the application of economics to health and health care.
In this post, we summarise the module and the topics covered. We also offer our own reflections on teaching during the pandemic in an online environment and hear what the students’ had to say about the module too.
Overview of the course and topics
When we first ran the course, we split the content quite equally between traditional health economics topics in the first half (health care demand and financing, economic evaluation etc), then the more health econometrics type topics in the second (health inequalities, mental health etc). This year, based on student feedback, we rearranged things a bit to incorporate some of the more empirical applications earlier on. This worked really well and we think we found a nice flow between topics.
The module begins by introducing health economics and the economics of health, their importance and some of their unique characteristics. It will introduce students to the theory of demand for health care including the Grossman model and its empirical applications, as well as individual health behaviour and the role of behavioural economics in health. Following this, it considers the financing of health care including health insurance and then explores inequalities in both the distribution and financing of health care, drawing on empirical analyses. The latter part of the module focuses on economic evaluation (EE) and decision-making relating to resource prioritisation within health care. It covers the methods involved in EE and explores its application in mental health and the role it plays in decision making in practice.
Specific topic structure
Week 1- Introduction to health economics
Week 2- Demand for health care and health
Week 3- Empirical evidence from the Grossman model
Week 4- Consumer choices about health behaviours
Week 5- Health insurance and health care financing
Week 6- Health inequalities
Week 7- Economic evaluation in health care and public health
Week 8- Applications of economic evaluation
Week 9- Economics and mental health
Week 10- The use of economic evaluation in decision-making
You will have to press play to understand why the photo of the flowers and bee on the first slide are relevant…
The impact of COVID-19 on teaching
The pandemic meant that we did not get to meet any of our students face to face, as all of the teaching was carried out online. We pre-recorded weekly lectures (split up into 3-4 20min chunks) and uploaded them at the same time each week. The tutorials were held via Blackboard Collaborate. For the tutorials, we asked students to submit short thought pieces before attending and then we split the group into smaller breakout rooms for discussions.
In terms of pre-recording the lectures, we felt this worked really well. It meant that students could work through the material at their own pace and stop and start the lecture at any time. Splitting the lectures up also worked well as it created clear ‘breakpoints’ in the content which may help with students’ revision.
Overall, the tutorials worked well, especially the use of breakout rooms to generate discussion amongst students. We did have some connectivity issues and we found it difficult to encourage the students to put their cameras on. We tried implementing the suggestions from a recent publication by Castelli and Sarvary (2020), but with limited success. Interestingly we also asked all groups ‘Would you have your camera on if everyone else had their camera on?’ and the majority said yes! It seemed we failed to establish a ‘cameras on environment’ from the outset and this is something we will try to change next year (if the tutorials take place in an online setting).
Some of the students also said that they felt Blackboard Collaborate was not the best environment for having cameras on because you can only ever see four people on screen at any one time. Whereas, applications like Zoom allow you to see all participants on screen. One student also suggested saying something like ,”Hey everyone, please can I see everyone who is able to, and comfortable with, turning on their cameras now”, in the very first session, then ask the students to introduce themselves with maybe name, course and where they are from.
Some student feedback (from our 2021 cohort)
“It was my first course on a more specialised economics topic (health), so it really opened up a new world of opportunities for me. Also really enjoyed the interactive tutorials.”
“The open structure of the pre-submission topic allowed to explore topics with regards to different countries and their health care system which was very valuable. The tutorials were well structured and resulted in the most discussion among students that I have experienced so far in online tutorials. Overall, I really enjoyed the course!”
“The course was really interesting and well structured.”
“The different areas of the course covered a lot about Health Economics. The online tutorials helped make them more interesting, although at times they have felt very forced. Tutorial participation points have helped however.”
“The lectures and tutorials were good. I also liked the grade breakdown 30% for essay, 10% tutorial and 60% exam.”
“The tutorials are surprisingly valuable. The attendance and homework grade also creates an incentive to stay on track which is really nice.”
Overall, it appeared that the students were happy with the content of the course and the way it was structured. In terms of the online setting, the consensus was that the online lectures worked very well but they would prefer to move back to in person tutorials.
Next semester (starting January 2022), we will be running the course again with more hands on deck from the Edinburgh Health Economics group! Specifically, Katharina and Giovanni will be joining Elizabeth (whilst Aileen takes a step back to focus on her other teaching commitments) to deliver another year of what will hopefully be a successful undergraduate Health Economics module.
At the end of April, Peter and Elizabeth, along with lead author Dr Catherine Hanna and patient representative Mr Steve Clark, presented their recent publication at the Power of Population Data Science Webinar Series.
Lucky for you, if you missed the webinar, you can watch it again on the Population Data BC YouTube channel here and see our slides from the event here.
The webinar was very well received with over 111 people signed up to the event and around 70 in attendance on the day. We were thrilled to spread the word about all of the hard work that has gone into creating this dataset, as well as all of the research we have planned so watch this space!
Within the UK, a standard approach to compare the cost-effectiveness of interventions has been established by decision makers like NICE. It relies on the costs to the NHS and social care balanced against difference in QALYs.
For several reasons, this approach falls short when evaluating interventions at the End of Life.
Firstly, a significant proportion of the important costs are likely be incurred outside of the NHS, the charitable sector, the welfare state, or the individual and their families and/or carers. These currently fall outside of a NICE standard economic evaluation.
Secondly, it is inaccurate to measure patient benefit since improved function is not expected. The standard methods for quantifying health outcomes is problematic in end of life care as the patient needs/focus are different than in those expected to improve.
Thirdly, the QALY is the recommended tool for capturing health outcomes across different clinical and disease areas. However, the ability of the QALY to capture aspects of health important to patients in an end of life context has been questioned given the aim at that juncture is neither improved survival nor function. The aims are to prevent and treat symptoms, preserve function, shared decision-making and family care.
As health economics informs decision-making, influencing the quantity, quality and sustainability of health care resources, it is imperative this methodology is applied to the highest possible standards.
For more information look at the Editorial “Incompatible: End of Life Care and Health Economics” by Katharina Diernberger, Bethany Shinkins, Peter Hall, Stein Kaasa, Marie Fallon published in the BMJ Supportive and Palliative Care here.
Historically, health economic research, especially economic evaluations and health technology assessment, have focused on physical health rather than mental health. This is partly explained by the difficulties in identifying and measuring mental health and its outcomes. A necessary first step before carrying out health economic research, is to describe and understand the size of the problem. Within the economics of mental health, this is a particularly difficult on account of both the invisibility of mental health and the historical stigma that has been associated with it, which has often meant that people don’t talk about their mental health. Although discussion about mental health has been growing over time for both sexes, their remains much to be explored particularly with respect to men’s mental health. Carrying out this exploration is vital if we are to design and implement effective treatments and policies that will have a positive influence on men’s mental health.
Are you a man interested in contributing to research on the subject of men’s mental health?
Trainee Counselling Psychologist Elspeth Quinn (equinn205@caledonian.ac.uk) at Glasgow Caledonian University is currently carrying out some of this exploration. Specifically, she is conducting a research project to investigate how men have experienced all-male social groups while suffering from depression. For this project, she is seeking male volunteers who have experienced depression in the past and would be willing to talk about this in relation to all-male social groups they have been a part of/are still a part of in their lives. This would involve a 45-minute interview at a convenient time via the online platform ‘Zoom’ that will be arranged over the next eight weeks.
The COVID-19 pandemic has had a devastating impact worldwide. Throughout the world, this impact has been felt especially in the long term care (LTC) sector. Edinburgh Health Economics (EHE) Research Fellow Elizabeth Lemmon has been working with colleagues from Scotland and the rest of the UK, on several pieces of work investigating the impact of COVID-19 on care home residents.
On 14th December, Elizabeth presented at a LTC-COVID-19 webinar with Professor David Bell, on the impact of the pandemic on mortality in Scotland’s care homes up until now. In this post, Elizabeth summarizes this presentation.
I’ve been working on some bits of COVID-19 research within the LTC setting since the beginning of the pandemic. The first piece of work was the Scotland report which is available on the LTC-COVID-19 website here. Next was the UK report, in which we compared experiences across the UK during the first wave. I’ve also helped produce the LTC-COVID-19 international report on mortality in care homes. Since then, like many other countries, Scotland has experienced a second wave of COVID-19 cases.
Before I go on to describe the mortality figures in Scotland, I think it is important to acknowledge the individuals who sit behind each of the figures. That is, individuals who have lost their lives, staff who have cared for them and families who have lost people who they love to this dreadful virus.
In total, as of the 6th December, there have been 5,868 confirmed or suspected COVID-19 deaths in Scotland. Of those, 2,393 occurred within care homes. That’s around 41% of all COVID-19 deaths. The chart here shows weekly COVID-19 deaths in care homes and weekly deaths from other causes in care homes. What we can see is the differing magnitudes between the first and second waves. Clearly, the magnitude of the second wave is much smaller, but nonetheless there is a visible increase in deaths during this period.
It is important to mention that these deaths do not include those care home residents who died outwith care homes. The data available in Scotland show that throughout the pandemic, there were at least 2,686 deaths of care home residents. That takes the total percentage of COVID-19 deaths accounted for by care home residents to 46%.There is a noticeable difference in this figure between the first part of the pandemic (16th March 2020 to 28th June 2020) and the second part (29th June – 6th December). In the former, this figure was 50% and in the latter it was 35%. This change might reflect that via the implementation of new guidance and policies, we have been able to partly protect care home residents during the second wave. These include more comprehensive testing strategies, which routinely test staff and residents.
Of course, these figures are conditional on the accurate recording of cause of death, which is a relatively strong assumption. Another way to measure the impact of COVID-19 on mortality is to look at excess deaths, that is the number of deaths over and above what would normally be expected. We define excess deaths as the percentage change in deaths compared to the previous 5-year average. In the peak of the pandemic, during week 17, excess deaths in care homes were 178% higher compared to the previous 5-year average. Throughout the pandemic overall, deaths in care homes were 25% higher. It is worth pointing out that recent evidence from the Lothian region of Scotland has found that among those homes where there was no outbreak of COVID-19, there were few non-COVID-19 related excess deaths (Burton et al, 2020).
Overall, like many countries, the impact of COVID-19 in care homes has been devastating. Some of the difficulties faced by the sector from the beginning of the pandemic included a focus from government of protecting the NHS. This meant that guidance and policies for care homes on testing and PPE were slower to respond. At the same time, a large number of older patients were discharged from hospital and into care homes during the first wave of the pandemic. Having said that, recent evidence from Public Health Scotland has demonstrated that these discharges had no significant impact on the likelihood of a care home outbreak.
The pandemic has exposed the urgent need for better LTC data in Scotland, even on a very fundamental level such as who lives in Scotland’s care homes. The pandemic has spurred on huge efforts to improve administrative data collection within the social care setting, especially those in care homes.
Whilst the focus of COVID-19 within the LTC setting has been on care homes, little attention has been paid to those older people who receive care within their own homes. In Scotland, around 47,000 people aged 65+ receive free personal care within their own homes (compared to around 36,000 adult care home residents) (Bell et al, 2020). At present, we know that their care has been adversely affected by the pandemic (Care Inspectorate, September 2020), but we know virtually nothing about how the pandemic has affected their outcomes. This presents a huge gap in our understanding of how COVID-19 has affected those in receipt of domiciliary care services at home. Evidence from England suggests that the proportional increase in deaths in the home care setting exceeds that of the care home setting (Hodgson et al, 2020). Again, better administrative data on those receiving care at home might help to address this gap in Scotland.
However, administrative data can only go so far as to truly explaining the devastating impact COVID-19 has had on so many lives. In order to provide this understanding, for example the impact on unpaid carers, families, front-line workers and more, survey data is required.
A couple of weeks ago, we posted a blog from Emma Wilson, an undergraduate economics student here in Edinburgh, who spent some time working with Edinburgh Health Economics on a voluntary internship during the summer. This week we hear from a second student, Georgina, who also worked on a project with EHE. Georgina shares a bit about what she worked on and reflects on how she found the experience overall.
Intern profile
Name: Georgina Cotterill
Bio: “I completed the EHE internship in the summer of 2020. I graduated from the University of Edinburgh having studied a MA Economics and completing the Health Economics module run by Aileen Neilson and Elizabeth Lemmon. I am now pursuing an MSc Health Economics at the University of York.”
Internship activities
“The aim of the internship was to write a paper assessing the variability of resource use data collection and costing methods in recent HTA-funded primary research papers. Ridyard and Hughes conducted a systematic review of all 100 UK HTA-funded primary research papers published from January 2000 to June 2009 in order to assess just this. They concluded that economic data is variable and a standardized approach should be adopted in order to improve transparency and external validity between studies. The aim of my work was to assess whether there has been improvements in the variability of resource use data collection and costing since 2009. Hence, I conducted a systematic review of a randomly selected 25 papers which fitted the following eligibility criteria: to be a HTA Journal, to be a primary research study, to be a randomised control trial (RCT), and written in 2019.” Paper available here.
“The results of this review display a high variability in methods used across papers and no considerable alignment since Ridyard and Hughes study of HTA-funded primary research papers from 2000 to 2010. HTA studies are still over-reliant on patient-completed forms which are costly and suffer from biases. HTA studies are lacking important data collection exercises, such as piloting and validating data collection methods. Such exercises are fundamental to ensuring reliable data collection. Additionally, the methods in estimating costs still lack transparency and are not fully documented on. Improvements and standardisation are still required in order to achieve good practice in data collection methods among HTA-funded primary research papers.”
Intern reflections
“The internship provided me with an excellent bridge from my undergraduate Health Economics studies to my Health Economics masters. As well as this, the internship offered me the opportunity to start thinking about what I had learnt about HE in a more applied and practical way.”
“I was unable to do anything related to the internship in person, due to the lockdown over the summer. This was a shame and it would have been great to go into the Usher Institute and talk to Aileen face-to-face. Of course, the lockdown affected many things and I am very pleased that I was able to do the internship at all.”
“I would absolutely recommend the EHE internship to others. If you enjoy and are interested in HE, this experience is a fantastic way of planning your career and / or further education and to verify what you really enjoy doing. It’s also wonderful to learn from experts in a field that you love.”
Project lead reflections
“I find it rather satisfying that the outcome of Georgina’s internship has been such a positive experience and that it appears to have been successful in allowing her to get to know if she really enjoyed health economics (after taking HE in the final year of her Econ UG degree) before committing to doing a Masters in Health Economics and picking up some transferable skills along the way. She did and she is! The latter currently at the University of York. Georgina was given a task, set of essential tools to investigate with, and the responsibly to produce her own bit work. She did very well in all aspects. Her exploratory review project of some recent literature on the subject of resource use data collection and costing methods used in more recent HTA-funded primary research provides a helpful ‘snapshot’ and ‘current state of play’, which would at least hint at that there may still yet be room to aspire to see further improvements in resource use data collection approaches, standardisation, transparency of reporting and good practices between studies… A much wider body of literature awaits to be explored! Well-done Georgina! All the very best for the future as your journey into health economics is only just starting. How exciting!” Aileen Neilson