Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
This summer, after running our first undergraduate Health Economics module, a couple of enthusiastic economics students approached us to ask if there were any opportunities to get some work experience with Edinburgh Health Economics. Whilst we don’t run any formal internship schemes, we thought we could definitely think of some useful projects for the students to get involved with. In this post, one of those students talks to us about the work that she did during her voluntary internship and offers some reflections on how she found the experience overall.
Intern profile
Name: Emma Wilson
Bio:“I recently graduated (virtually!) in Economics from the University of Edinburgh in July 2020 and I am currently working as a Competition Economist for the Financial Conduct Authority. I have had a strong interest in Health Economics since I started working for the NHS in the first year of university in the holidays, and I then took the Health Economics course in fourth year solidifying my interest. My interest resulted in me writing a health/labour market dissertation about gender differences in wages due to health.”
Internship activities
“During my internship I have been working on part of the CORECT-R project. The project aims to create a UK wide Colorectal Cancer Intelligence Hub and identify the opportunities to impact on care to improve outcomes across the UK and provide evidence to guide interventions that will minimise inequalities and improve survival. I have specifically been working with Dr Elizabeth Lemmon on a report on costing methodology heterogeneity called ‘Validating costing methodologies used in the health economic literature of colorectal cancer’. You can view the report here.
The report looks at a cross-section of 20 papers of the most recent health economics literature on colorectal cancer. The studies are compared and contrasted against not only one another, but also against costing methodology criteria that has been laid out in a previous study on costing in health economics. It is concluded that due to ambiguity around costing methodologies and I suggest several ways in which the transparency around costing can be improved: studies should explicitly state whether they use micro, gross, top-down or bottom-up costing, providing clear evidence of how they do so; studies should also provide clarity in their computations and clearly state cost sources, and the identification process of costs used should be made clear. I suggest at the end of my report that a CHEERS type checklist for costing should be created in the future to ensure that costing methodologies are more homogeneous and allow for studies to be easily replicated and generalised.”
Intern reflections
“During my internship my critical literature analysis skill have increased hugely from examining a large number of academic papers and examining them. My academic writing skills have also improved from the constant feedback loop I have had with Dr Lemmon. The autonomy that I have been given to work on the project has been something I have never had before, and I have enjoyed the accountability I have been able to take for my work. The internship has been a great opportunity, and I would highly recommend it to anyone else with an interest in health economics, or in improving their analysis or academic skills.”
Project lead reflections
“From our perspective, it was brilliant to have Emma on board to help with the costing methodologies used within the health economics literature on colorectal cancer. This is an area in which we have found significant heterogeneity and Emma’s work confirms and documents this. Her work will be extremely helpful for the project going forward. Overall, Emma was a pleasure to work with and she has really set the bar for future ‘interns’!” Elizabeth Lemmon
Our Research Fellow, Elizabeth Lemmon, has been contributing to several reports on the impact of COVID-19 within the long term care (LTC) system in Scotland and around the world, with colleagues from the University of Stirling, Edinburgh Napier University, London School of Economics and the Bruyère Research Institute. These reports are being produced for the Long Term Care Policy Research Network’s newly established LTC responses to COVID-19 platform, which aims to:
Document the impact of COVID-19 on people who rely on long-term care (including unpaid care) and those who provide it.
Share information about policy and practice measures to mitigate the impact of COVID-19 in long-term care and gather evidence about their success or otherwise.
Analyse the long-term implications of this pandemic for long-term care policy.
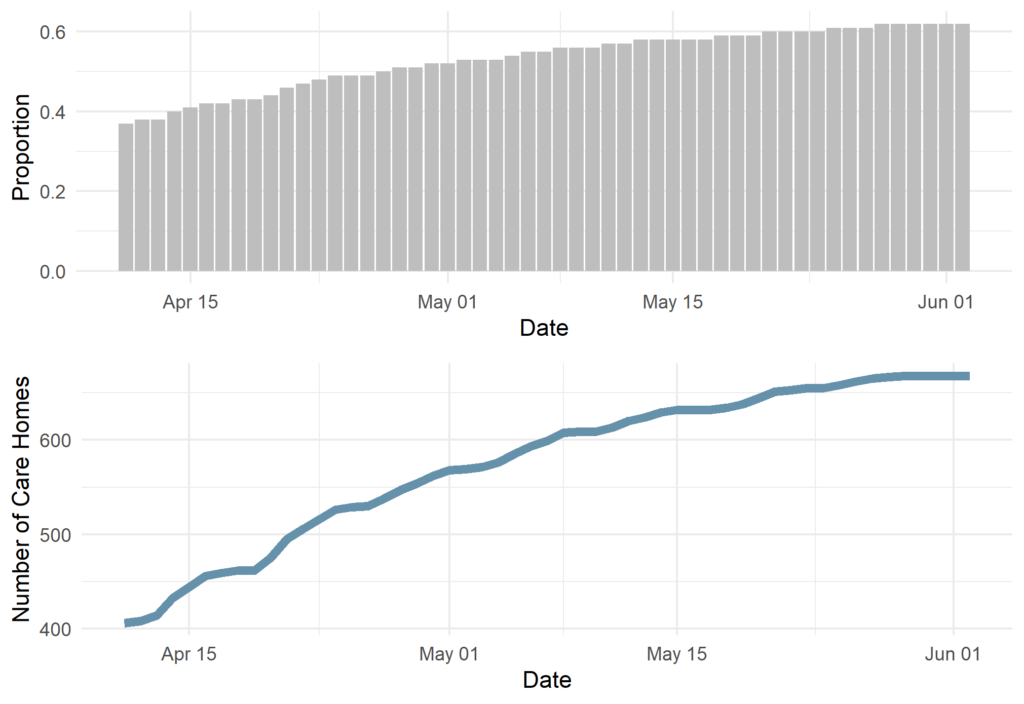
The Scotland report – available here – focuses mainly on the impact of COVID-19 within Scottish Care Homes, where the impact has been particularly devastating. At the most recent release of this report (3rd June), around 47% of all COVID-19 deaths occurred in care homes. Furthermore, as shown in the figure below, more than 62% of all Scottish care homes had reported at least one outbreak of COVID-19.
The International report – available here – also focuses on care homes and care home residents, but aims to draw comparisons between countries around the world. This is incredibly difficult due to the different geographical, demographic and political contexts, which is further complicated by significant differences in the recording of data. The report highlights the key difficulties associated with mortality recording and the need to use data on all care home residents and not only those occurring within the care home.
Both reports are live documents that are being updated as new data become available. Elizabeth is also involved in a new report which is currently underway on the UK situation. This report hopes to draw useful comparisons between the four UK nations.
The COVID-19 pandemic has meant that, along with the rest of the academic community, our team here at Edinburgh Health Economics (EHE) have also been learning to adapt to a life of working from home. In this post, we wanted to share some of how we have adapted, what we think we have learned so far, as well as some of our top tips for #WFH.
On 23rd March 2020, the Prime Minister announced that the UK was being placed on a nationwide lockdown. At this point, we had already fetched our belongings from our office in Edinburgh’s BioQuarter, and had a slight head start in the transition to #WFH life.
We of course all looked to Andy – who normally works from home a few days a week anyway – for the top tips! His number 1 top tip was to do whatever possible to maintain a “professional mode” mind-set during work hours, and differentiate it from personal time. This might mean getting up at the same time as you would for travelling to work, doing things like having breakfast before starting (not at the desk), wearing my work clothes and working through a daily task list like it’s a schedule. Without the commute, Andy said he finds he can put in more time working and have more spare time as well. The “Free Lunch [break]” may be less apocryphal than its namesake!
Pete very quickly got the EHE team set up on Microsoft Teams and we decided it would be nice to have weekly video call catch ups on there. We don’t structure those meetings, they are just for general chit chat. Mostly we talk about what we did at the weekend and Katharina shows us what she sketches she did the night before at her life drawing class. Overall, the catch ups serve as a good reminder of what day it is and help maintain some sense of normality in what are very abnormal times.
We also hosted our first internal academic seminar on Teams with one of the new EHE PhD Students, Jo Mair. The seminar was a complete success! The screen sharing feature of Teams made it easy for Jo to share her slides with us and we could also share resources with her on the chat at the same time. We’ve scheduled our next two academic meetings to take place on Teams later in June and July. If anything, being forced to use Teams and hold the video call seminars has made us think about inviting speakers from further afield to talk to us about their research, both broadening the choice of speakers and helping the environment at the same time! The adoption of MS Teams is having other workflow benefits – we find it easier to use for video conferencing than Skype and it integrates will with other parts of our workflow using Office 365 and Trello.
Some of us were perhaps better geared to work from home than others, so our transitioning trajectories have differed slightly. As we mentioned, Andy is an old-timer when it comes from #WFH, so he was way ahead of everyone else. Aileen, (another ‘old-timer’, but for different reasons!) has for pretty much all of her working life to date, only really known a routine which involves going into the office on most days, so for her, moving from working at home say on 1 day a week to 5 days has taken a bit of getting used to. Elizabeth has never lived without her desk somewhere nearby, so after investing in a keyboard to use instead of her lap top keyboard and hooking up an old TV monitor to use as a second screen, she was all set. Alistair transformed his spare room and purchased some gadgets to make video calling possible. Katharina had recently moved into a new flat and being the avid outdoor mountain climber, hiker and cyclist that she is, the suitability of the flat for #WFH didn’t feature when she signed the lease. So for her, the adjustment to working at the dining room (and living room and kitchen) table has possibly been the hardest. Pete is lucky to have a garden and has taken the opportunity to adapt this through the addition of some flowerbed-based bike tracks (and has started work on a wildlife pond. Holly set up a #WFH work station on the top of a piano (which is better than it sounds). The main complicating factor of #WFH life in lockdown has been juggling work with care of 2 four year olds in shifts with her partner.
EHE Lead Pete is still working in clinics at the Edinburgh Cancer Centre, making sure that his patients are well looked after and also checking in on the EHE team. Our hats go off to Pete and all of the NHS and social care staff who are continuing to look after those who need it at this very difficult time. This has the knock-on effect of our team becoming more self-reliant, helping us to work together to move projects forward with autonomy and bottom-up innovation.
We’ve asked each person in the EHE team to give us their top tip for #WFH and to answer another #WFH related question. We hope these are helpful to you either because they give tips you hadn’t tried or they just remind you that we are all in this together
What’s your top tip for other academics who are #WFH? I think if I am honest my best piece of advice is simply to try to develop a new WFH ‘routine’, as best you can – this might sound a bit non-prescriptive, but adapting in such a way that works best for you / your family / home situation in what are and continue to be quite challenging times in many folks lives I imagine. For me, this has meant adapting and planning my working day in a different way, but trying to keep essential and familiar elements to the working day as well – just as I used to have my non-WFH work day routine, getting up at the same time, leaving home for the ‘walk’ / commute going into the office (exercising in the morning instead before work or a lunchtime run or walk etc. just helps keep ones physical/mental health/ wellbeing ticking over!…). Then trying to finish up work as you would normally end the day, winding down for the ‘journey’ home – usually another walk for me (which we can take more of now!).
What do you most look forward to when returning to the office? The ‘new normal’ – makes me wonder what life (working and non-working) could look like once coronavirus lockdown is eased. How will we, work (more working at home?), educate (more on line teaching courses?) and travel (more walking, cycling?). I think what I am most looking forward to when returning to the office is ‘seeing’ my EHE colleagues again face-to-face (other ECTU unit and wider Usher Institute ones as well).Though, it has surprised me how well we seem to have acclimatised to using /MS teams or video calls for meetings etc., and I think we will keep using this flexible technology function to some extent going forward.
What’s your top tip for other academics who are #WFH? I am find that I am easily distracted from work and have always benefited from being around productive people. With me in my home and my colleagues elsewhere I have had to find other ways to improve my productivity. My solution has been to install plugin on my chrome browser called StayFocusd, which counts the amount of time I can spend on websites I have told it I tend to procrastinate on.
What’s been the biggest challenge when adapting to the #WFH set up? The biggest challenge to me has been finding ways to get the benefits I am used to getting from face to face interaction with my colleagues. Although there is no true substitute or talking in person I was able to improve my video call experience. I was previously using my phone for video calls as I could not find any webcams to buy online. I was therefore limited to my phone screen and was unable to share my computer screen during meetings. I managed to download an app for my phone called EpocCam which allows me to use my phone camera as a webcam with my PC over WiFi. I also ordered a desk microphone so others would be able to hear me more clearly and my girlfriend could join me for informal video calls.
How has your productivity been impacted from #WFH? I am find that I am easily distracted from work and have always benefited from being around productive people. With me in my home and my colleagues elsewhere I have had to find other ways to improve my productivity. My solution has been to install plugin on my chrome browser called StayFocusd, which counts the amount of time I can spend on websites I have told it I tend to procrastinate on.
What’s your top tip for other academics who are #WFH? As well as the tips above, I think staving off distraction is important. It’s perhaps obvious, but no TV. Less obviously, keep the desk area tidy, particularly the area in vision when working. Less clutter means I’m more relaxed and focussed, so the first thing I do each day is tidy up while the kettle boils. This (and the coffee!) also offers a one of the best rates of return on investment in terms of full time equivalent work added to satisfy the economist in me.
Home set up has made a big difference to both comfort and productivity as well. Avoid hunching over coffee tables from sofas, it’s very bad for your back. You want a proper desk or dining table surface. I also use an old TV connected by HDMI cable as a second monitor, and a spare tablet as an all-purpose correspondence device for email/MS teams or video calls. If like me your spouse is furloughed, some way of indicating when not to pop in to get something from a cupboard helps a lot. Asking if you can use the same system to request cups of tea, is much less advisable.
Any tips for keeping physically active when working from home? My biggest tip is to walk around your house whenever you’re on a call that doesn’t need you to be at a computer. I use a hands-free kit and essentially circle my living room clocking up steps. A half an hour phone call can be 2,000 steps easily, and a few of those in the day (including conversations with family on the evening) will add up very quickly. You can also do this in short bursts anytime you are stuck writing something and need to think. More recently I added an under desk peddling machine. Its early days but so far it has been really good. I need to sit slightly back from my desk to use it so it’s no use when typing or coding, but it can be used when on vid calls and sharing screens etc, and works very well when reading or dealing with quick queries like emails. My last tip since home exercise equipment is hard to get a hold of, is that old water bottles can be used as dumbbells. 1 liter = 1kg thanks to the metric system, so that old 2 litre bottle of cordial with the really thick plastic and hand grip spaces on the side can be a 2kg one if you need it.
What’s your top tip for other academics who are #WFH? This might sound bizarre, but it is to wear your shoes at your work station (make sure they are clean of course)! I’ve read a lot about top-tips for #WFH and lots of them say get dressed for the day as you would for work. I don’t tend to dress any differently for work than I do for the weekends or evenings. So for me, my attire doesn’t make me feel more like I am working. But what does help are my shoes! If I wear shoes at ‘work’, I can take them off when work is finished and it feels more like I’m able to separate work and home.
How have you been looking after your physical health? I’m very physically active normally, though I rely on a lot of equipment, so maintaining my fitness has been a challenge without access to the gym. Having said that, I’ve managed to come up with lots of home workouts and a new bike that I got for my birthday has helped. I do find I am slightly less motivated to push myself but I am trying not to be too hard on myself. I’d say that doing small bits of exercise often is the best way to do things.
What’s your top tip for other academics who are #WFH? I worked from home for a period in the past and my advice this time around is a little different because of my circumstances. My partner and I both work full-time, I teach part-time and we have two four year olds who are normally in nursery – in a 55m2 apartment. At the start of lockdown we drew up a shift schedule alternating set uninterrupted times in the mornings and afternoons, with evening shifts added in during the week. I try to get work involving phone calls, email contact and meetings done during the daytime shift, with the evening shift free for reports and work that isn’t reliant on others being online. It is far from ideal but I can’t think of any other way of managing at the moment and it feels as sustainable as any model we’ve come across. I’m outside a lot with the children (community allotment, river bank, woods, shared gardens) during my stints and we started out building in exercise for us (running or cycling) early in the morning or last thing at night but it’s unfortunately the only thing I can take out of the equation when I get tired – plus reading. I’m normally an avid reader but haven’t read much at all since lockdown began. I have, however, joined a coffee subscription scheme.
What do you most look forward to when returning to the office? The first thing that comes to mind is the office itself. That will mean that we have some childcare in place and the ability to travel into the office to work, which also includes a bike commute that I really enjoy. I suspect at this point that colleagues will be able to go back to the office in small groups or on rotas before we have consistent childcare back in place. I think I can work well at home but, in the current set-up, my productivity is not great. On a more positive note, the experience of lockdown has moved the use of technology for meetings, office work and seminars on in leaps and bounds. I suspect I am more confident now and it will be easier to make a case going forward for online training and meetings rather than travelling for hours for physical meet-ups.
What’s your top tip for other academics who are #WFH? My approach to working from home is going slightly against some of my colleagues recommendations and I am honestly not sure it is the best advice – anyway it works for me. I am in sports clothes all day and tend to break up my days doing multiple 5-10 minute fitness challenges in-between different tasks. This helps me to take short breaks, which is essential for me to stay focussed -I feel that I will very much miss that opportunity once we are back at BQ9. I find myself starting to work quite early in the morning as I am more focussed and the systems I am currently working with seem to be less frequented and therefore more reliable. I try to organise some activities for the evenings in order to make sure to stop working and focus on something else. My top tip definitely is to be nice to yourself, give yourself credit for finished tasks and get yourself cake, ice cream or whatever motivates you!
How have you been looking after your physical health? I am a very active person with plans for nearly each evening and admittedly struggle to get the level of socialising and sportive activities necessary to feel balanced. I frequently combine being active with meeting friends which I try to keep up in a modified form. I am challenging (and being challenged) by several friends to do a variety of fun and crazy fitness challenges, I am currently doing a 30-day yoga challenge, I am having hangboarding sessions with some climbing friends and I am walking a dog.
In this post, written for the Early Career Researchers Using Scottish Administrative Data (eCRUSADers) blog, Catriona Keerie, Senior Statistician within Edinburgh Clinical Trials Unit (ECTU) talks about her work within ECTU and her involvement on a rare Scottish trial that used administrative health data. She provides some great diagrams to help along the way, which I can tell you are essential if you want to understand the complicated structure of the data! Catriona also highlights some of the key challenges the team faced in terms of data access and use and offers her reflections on what they learned from the project which could help other trials like this one in the future.
Can you tell us a little about your role in ECTU?
My role involves a variety of tasks – however, primarily my role is the statistical reporting of trials run from within ECTU. I typically have up to eight active trials throughout the year. My role varies on these – I am Trial Statistician for approximately half of them, and the ‘reporting’ statistician for the other half. When I have my reporting statistician hat on, I’m responsible for the statistical programming and generating the analysis and results.
How trials have you worked on that have involved using administrative data?
Since I joined ECTU in 2014, I have worked on three trials using administrative data. Two of them used solely routine healthcare data and the third one is running currently, based on a blend of routine data plus data captured within the trial.
Is the use of administrative data in trials becoming more common over time?
The use of administrative data in the trials setting is definitely becoming more common since clinical trials are known to be expensive and time-consuming. The use of administrative healthcare data is viewed as a more efficient means of understanding the health of the population using readily available data. However, there is a trade-off in terms of the quality of the data being captured.
It’s a relatively recent study design that’s increasingly being used to evaluate service delivery type interventions. The design involves crossover of clusters (usually hospitals or other healthcare settings) from control (standard care) to an alternative intervention until all the clusters are exposed to the intervention. This differs to traditional parallel studies where only half of the clusters will receive the intervention and the other half will receive the control. This diagram helps to demonstrate the difference in designs:
The population of interest were patients presenting in hospital with heart attack symptoms. The trial sought to test a new high-sensitivity cardiac troponin assay against the standard care contemporary assay. Specifically, to test if the new assay could detect heart attacks earlier and with a more accurate diagnosis.
How were patients enrolled into the trial and how does this differ from a standard trial?
Step wedge trials usually randomise at a cluster (hospital) level, rather than randomising patients individually, so this was the main difference to a standard trial. So patients were enrolled rather than randomised into the trial. Standard trials require patient consent before randomisation, but in this context, individual patient consent was not needed due to the randomisation being performed at hospital level. Appropriate approvals for consent were sought through the hospitals.
If patients presenting with heart attack symptoms at any of the hospitals were eligible for the trial (based on our pre-specified inclusion/exclusion criteria), then we had permission (at hospital level) to include them in the study and use their securely anonymised data.
How many patients were enrolled into the trial?
Approximately 48,000 patients were enrolled from 10 hospital sites in NHS Lothian (3 sites) and NHS Greater Glasgow and Clyde (7 sites), over a period of just under three years.
Which administrative data sets were used?
We used a total of 12 distinct data sources which were a combination of general administrative datasets and datasets more specific to our area of research from locally held electronic health care records. Prescribing data was obtained from the Prescribing Information System, also ECG data, plus general patient demographics. Trial-specific outcome data was obtained from the Scottish Morbidity Record (SMR01) and also from the register of deaths (National Records of Scotland). All data were captured separately for each Health Board – there is currently no amalgamated data source which holds all data. Health Boards are the owners of their own data.
The main linking mechanism for these 12 data sources was the patient CHI (Community Health Index) number. To ensure patient anonymity, CHI numbers were securely encrypted prior to use.
How did you get approval for these data sets? How long did this approvals process take?
Approvals were required at a number of levels. We required ethics approval, approval to use patient data without consent and Health and Social Care approval (through the Privacy Approvals Committee, predecessor to the Public Benefit Privacy Panel). There were also health board specific approvals required for local data to be released. In addition, we required data supplier approval. Finally, approval was needed for the data to be hosted on the Safe Haven platform.
This process was long! This was ongoing throughout the duration of the trial. Although the data was being captured automatically via routine records, the final dataset wasn’t confirmed until relatively late on in the process due to complexities of mapping locally held healthcare records. One of the advantages of the national datasets is that they are the same across all health boards.
Where were the data sets stored?
Datasets from NHS Lothian and NHS GG&C were supplied separately in their own Safe Havens. The combined dataset was hosted on the NHS Lothian Safe haven space on the National Safe Haven analysis platform .
How did the linkage of the data sets happen?
The data sources from both health boards were combined and hosted on the National Safe Haven analysis platform. This wasn’t a straightforward process. Although we’d anticipated capturing exactly the same patient data across both health boards, the reality was quite different.
Data were captured in different formats with different variable names and different definitions. So there was an unexpected element of data cleaning required before the data could effectively be merged into one large analysis dataset.
The final linkage was done using the securely encrypted CHI number for each patient.
What do you see as the major benefits of using administrative data in this setting?
Use of administrative data in this context is a more efficient process – less resource spent on the administrative aspects of trial enrolment e.g. capturing demographic details such as age, sex, postcode or medical history.
Using administrative data also gave us the opportunity to research a large representative patient population in comparison to the setting of an RCT where a strict pre-specified population, not necessarily representative of the target population, are studied.
Overall, what were the major challenges of the study?
From the data side of things, ensuring the correct data was extracted was difficult. The diagram above is very over-simplified view of what happened! The reality of picking up the required variables from two separate health boards which capture data very differently was difficult.
Another challenging aspect was ensuring that a patient wasn’t enrolled more than once in the study. Patients can present in any hospital with heart attack symptoms more than once, so we needed to ensure they weren’t included in the study each time they came to hospital. This required a de-duplication algorithm using encrypted and de-identified patient data.
However, I think the biggest challenge was for those in the team tasked with obtaining the correct approvals. It was underestimated how complex this would be. While approval for the national datasets was straightforward and the eDRIS team were very helpful, processes for locally held data at the time of trial set up were not established. Legislation around patient data confidentiality was continually changing, so we were faced with keeping abreast of new legislation as time progressed. The safe haven networks are now more established and hopefully, the processes are more straight forward.
Is there anything you would do differently next time?
I think the data validation aspect of the trial is crucial. Ideally we would have had more time spent on this in order to ensure the data was as correct as possible. Involving the clinical team much sooner in this process would have helped – they have a really important role to play in terms of ensuring the data picked up makes sense from a clinical perspective.
For High-STEACS, the access to the data was highly restricted and did not include the clinical team. Many of the data discrepancies were only picked up at the final review stage once data and results had been released out of the Safe Haven area.
Working within the Safe Haven environment creates time lags on both sides of the process – data being imported into the Safe Haven and also results exported out at the end take time. We hadn’t considered this time lag when working to tight timelines.
Do you know if anyone is using the learning from this trial for future trials of this kind?
The High-STEACS trial was directly followed by the HiSTORIC trial, addressing similar research questions and using many of the same data sources. So we have been through the loop again which has made for a more streamlined process. Other trials within ECTU are also making use of the learnings from High-STEACS, particularly from the governance and approvals side of things.
Summary
Thanks for sharing this with us Catriona! It is great to see that administrative data are being utilised alongside clinical trials in Scotland. It is also interesting to hear that despite being part of a trials unit like ECTU, the High-STEACS team still faced many of the same challenges that researchers and eCRUSADers have experienced when using administrative data for research. In particular, we can relate to the issues of permissions, timing and working within the Safe Haven environment. Overall, it seems that the timing issues were due to the use of the locally held data rather than using the national data.
Hello, my name is Jo and I am undertaking a part time PhD within the Usher Institute, my supervisors are Dr Nazir Lone, Dr Peter Hall and Professor Kev Dhaliwal. I currently work for the Centre for Inflammation Research as a Clinical Project Manager within Professor Kev Dhaliwal’s team and have done so for the last 6 years. To date my further education consists of an undergraduate degree in Pharmacology, a MSc in Bioinformatics and a MSc in Public Health Research.
I have worked for the University of Edinburgh for the last 13 years in various roles within research. These include working in a clinical research facility, a research and knowledge exchange office and in research governance. I also have experience working within the NHS in clinical trials. Prior to that I worked in various ad hoc roles and travelled/worked in South America, New Zealand and South Africa (some photos below!). I have been a member of the NHS Research Ethics Service for nearly ten years, being a member of SESREC 2, then the chair and I now sit on Scotland A.
The group I work within focus their research on respiratory disease and the ways in which diagnosis of respiratory disease can be improved. Whilst working within this group I have been able to get fully immersed in translational research. Day to day working can involve anything from writing protocols and regulatory applications to being in the laboratory building medical devices, being in the clinics and wards assisting the clinical staff with study participants, negotiating commercial contracts for third party outsourcing, dealing with finances and creating structures and processes for forging our way through unknown territory and getting novel compounds and devices into man.
One area the group is researching is looking at fast, bedside, point of care diagnosis of pneumonia and identifying the gram status of the infection in ventilated patients. The group have developed a novel diagnostic technique consisting of an imaging system, compounds that allow diagnosis of lung infection and a delivery device to deliver the compounds into the distal lung. Work is currently underway to pilot the novel technique leading to a second stage clinical study within Edinburgh and three other UK sites.
PhD Motivation
Whilst working within my current research group within the media of novel developments to improve health, I became more aware of the difficulties in pushing research through to a stage where we can get it into the NHS. Gathering evidence of the impact a novel diagnostic tool could have on the NHS and the lives of patients is a time consuming and arduous process. Whilst most people appreciate the necessity of ensuring a diagnostic test is safe and does what it intends to do, perhaps measuring the potential impact on the patients and the NHS could be done in more than one way? Increasing evidence and developments support this way of thinking. The availability of observational data is increasing all the time and the skill set to put it to use expanding. As such I finally felt I had a focus I could put towards a PhD! With amazing help and input from Dr Nazir Lone, great support from Professor Kev Dhaliwal (and team, especially Dr Anne Moore) and invaluable time with Dr Peter Hall I developed the outline of a workable PhD, applied for and obtained a staff scholarship.
PhD Plan
Within my PhD I will be looking at the use of the observational data from ICU patients and how this can be used to model the potential impact of a novel diagnostic on patient outcomes and NHS (costs). I would ultimately like to compare this to the data being gathered as part of the clinical study to see how the observational data can add value to or replace some aspects of the clinical study. Initially, I am focusing on developing the care pathway map within ICU for patients with suspected pneumonia, gathering the necessary data (through extraction from NHS systems into a safe haven plus utilising other data sources/sets), assessing where the novel device could be most useful and comparison with the reference standard as developed through the clinical study. With regards to the health economic modelling I am working towards the construction, parameterisation and analysis of a health economic decision model based on the care pathway developed. The model will initially calculate expected costs and outcomes for the current care pathway. The new diagnostic test will then be incorporated into the model at key decision points, as indicated by the current evidence and recommendations from the specialist advisory group (for the clinical study). Divergence in the clinical pathway consequent on test results will be modelled based on the diagnostic properties and decision impact of the test.
I have entered into discussions about PhDs in the past and could never quite commit myself but I really feel this one ties in with my work and the group’s ethos whilst being interesting and worthwhile. I’m enjoying it so far, between this, work and living the fairly quiet life in East Lothian (Drem), if you can call having three young daughters (pictured with me below) a quiet life – it all keeps me rather busy!
Last week, Elizabeth was invited down to St Andrews House to present her PhD work to the Health and Social Care Analysis team. Specifically, this presentation covered her PhD research on the provision of long term care to older adults in Scotland, with a particular focus on the usefulness of Scotland’s administrative data (data that are collected routinely as part of service provision) in answering her PhD questions. In this post, Elizabeth gives you a quick overview of her presentation.
You might be wondering why there is a photograph of me (top right), my mum (top left) and my grandmother (centre) at the top of this post. As well as showing the increasingly familiar image of a multi-generational family (my mum might prefer if there was another generation in there but I have told her she is going to have to wait a few years for that!), I like to use this photograph to tell the story of my PhD. So here goes….
Paper 1: Variations in domiciliary free personal care across Scottish local authorities
Data used: Social Care Survey (SCS) and other publically available, area level data sets
This paper looks at things from my Grandmother’s perspective as an older person who is receiving personal care services. In particular, it explores variation in the provision of Free Personal Care (FPC) across Scottish local authorities, in order to establish whether or not FPC provision matches the need of the population.
Paper 2: Utilisation of personal care services in Scotland: the influence of unpaid carers
Data used: Social Care Survey (SCS)
This paper looks at things from my mum’s perspective as an unpaid carer who is providing care to my Grandmother. In particular, this paper uses the SCS to try and understand how unpaid carers can influence older people’s use of personal care services.
Paper 3: The cost of unpaid care: a standard of living approach Data used: Family Resource Survey (FRS)
My final paper looks at this from my perspective, as an onlooker to the caring situation going on between my mum and my Grandmother. This perspective asks, “who cares for the carer?”. The aim of this paper was to understand whether or not unpaid carers experience a reduction in their standard of living due to caring, if so then how much would they need to be compensated by in order for them to reach the same standard of living as a non-carer, and finally how would that level of compensation compare to the current Carers Allowance.
If you want to know what I actually did and found in each of these three papers, you can have a look at my thesis here.
My PhD and Administrative Data
I had planned to use a national, linked administrative health and social care data set for my PhD. In fact, I applied for this in April 2016. Unfortunately, I didn’t get access to it until April 2018 and by this point I had had to come up with a plan B and was running out of time/funding to be able to get to grips with the linked data.
As a result, I made do with publically available, geographical level data, survey data and administrative social care data.
Did the administrative data help? Some reflections…
Well yes, of course they did. I was able to do some pretty cool work in my PhD using the SCS and this wouldn’t have been possible without it. However, the PhD really taught me that the administrative data struggle is real! A few things I highlighted in the presentation to the Scottish Government were:
Approvals process and linkage timing. Two years is simply too long in the lifetime of a PhD and I did not foresee that it would take this long.
Administrative data aren’t designed for research- they typically lack important controls that we really want/need in econometric analysis. But if we want to answer policy relevant questions with administrative data, surely they should be designed with this in mind? See this recent blog post I did with my colleague from Napier for the Office of Statistical Regulation.
There were lots of differences between local authorities in terms of data recording, missing information etc, which can cast doubt on the conclusions (of course I have carried out as many sensitivity and robustness checks to ensure this isn’t the case, but there is still doubt).
There isn’t any information about the unpaid carers in the SCS. Again, this is important information that is lacking from the administrative data.
Sadly, I’m still enduring this administrative data struggle in my role here in Edinburgh Health Economics. In an attempt to do something about this, I have spent some time developing a new platform called Early Career Researchers Using Scottish Administrative Data (eCRUSADers). I’m hoping that this will reduce the struggle for any researchers who are new to the administrative data scene. You can find out more about eCRUSADers (or join us?!) on the website here.
View of Calton Hill from the conference room at St Andrews House.
The PRC is a European Research Centre consisting of 17 international and 8 national collaborating centres. They plan and conduct international multicentre studies within palliative care, focusing on pain, cachexia and health care services. On the 30th January, the TVT (Two Versus Three Step) study, primarily run by the centre in Edinburgh, presented the initial clinical and health economics results at the PRC Seminar in Oslo ahead of the main results being published.
The TVT Study “An international, multicentre, open randomised parallel group trial comparing a two-step approach for cancer pain relief with the standard three-step approach of the WHO analgesic ladder in patients with cancer pain requiring step two analgesia” recruited patients in the UK, Mexico, Uganda and Israel and was comparing the 3-step approach for pain control currently recommended by the WHO* to a 2-step approach omitting weak opioids.
The primary outcome was time to achieving stable pain control, where stable pain control was defined as the first day of three consecutive days with average pain score ≤3 on a numeric rating scale of 0-10. The trial also looked at a potential increase in opioid-related side effects.
This was a very interesting trial from a health economic viewpoint, taking into account the different costing systems within the participating countries. Though the quality of life component (EQ-5D-5L) was captured in all countries, a full economic evaluation was only possible for the UK as the country specific value set was readily available.
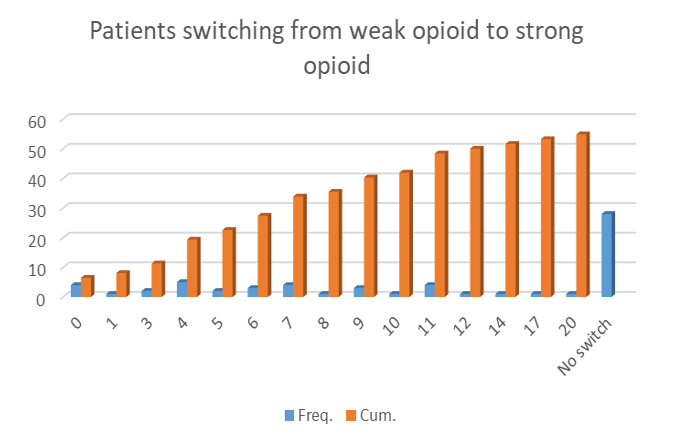
The main results of the study can be summed up fairly quickly – omitting step 2 (weak opioids) showed no significant difference in terms of pain control, lead to a reduction in opioid related side effects, is cheaper and patients -reported better outcomes for quality of life. Further to this, more than half of the patients who started on a weak opioid had to switch to a strong opioid in order to achieve pain control. The link to the full publication will be added as soon as the results are published.
Figure 1: Preliminary results from the TVT study. Number of Patients who needed to switch from a weak to a strong opioid within 20 days.
The introduction of the presentation highlighted the importance of health economics within palliative care (as a main tool for decision making within the health care sector) and tried to clarify misconceptions about health economics. It focussed on the challenges we are facing in terms of collecting costs, measure patients’ quality of life and putting a value on “life improvements” in this particular setting. This part of the presentation facilitated interesting discussion at the conference and some ideas for possible future collaborations.
After the seminar I stayed in Oslo for the weekend to catch up with friends and use the opportunity to visit the Henie Onstad Art Centre in Oslo which is currently hosting the “Picasso 347” (below), and “Claude Monet and Bærum” exhibitions as well as “Yayoi Kusamas’ – Hymn of Life” (at the top of this post). I can highly recommend a visit!
*WHO 3-step-approach:
Step 1. Non-opioids (non-steroidal anti-inflammatory drugs [NSAIDS], acetylsalicylic acid [ASA, aspirin] and paracetamol [acetaminophen]) for mild pain.
Step 2. Add an opioid for mild to moderate pain (Codeine, Tramadol).
Step 3. Add opioid for moderate to severe pain (morphine) titrated to pain relief or alternatively to occurrence of dose-limiting adverse events (AE).
Aileen joined Edinburgh University’s Usher Institute and Edinburgh Clinical Trials Unit (ECTU) as a Senior Health Economist in 2018. Aileen’s current role includes leading and developing health economics research in The University of Edinburgh and NHS Lothian, contributing to the development of new methods and techniques in health economics through methodology research embedded within applied studies e.g. Randomised Control Trials and other study design. She has experience in conducting and managing health outcomes research and economic evaluation studies in the UK NHS setting and other European countries.
She holds a BSc in Science with Management Studies (Napier University, Edinburgh) and an MSc in Operational Research (Strathclyde University, Glasgow). Prior to joining ECTU Aileen worked as a Research Fellow with the Health Economics Research Unit, Aberdeen University (HERU) for 5 years. She has worked in various clinical areas including oncology (prevention/screening/detection/treatment), orthopaedics and trauma surgery, intensive care, stroke, rheumatic and musculoskeletal diseases and chronic pain. She has 25 years of prior research experience, in academia (e.g. Universities of Nottingham, Dundee, St Andrews, York, Aberdeen), the NHS (Lothian – Primary and Community Care Division) and in health care consultancy roles (e.g. HealthEcon AG, Basel, Switzerland, and the Norwegian Knowledge Centre for the Health Services, Oslo, Norway incorporated in the Norwegian Institute of Public Health as of 1 January 2016).
Research Interests
Aileen’s research interests are broad, spanning both developing and applying trial- and model-based economic evaluation methods of different interventions/technologies. She is particularly interested in economic evaluations of public health interventions, and research that focuses on the (improved) use of routine administrative data for cost and outcomes measurement in undertaking heath economics analyses/ economic evaluation studies.
Aileen is currently the course organiser for the “Introduction to health economics and resource allocation” elective course on the Masters in Public Healtj (on-campus) which ran for the first time in 2018/19 and is currently running for 2019/20. Aileen also teaches alongside our Research Fellow, Elizabeth Lemmon, on the new undergraduate module on Health Economics which is being offered for the first time in the School of Economics. She also supervises masters’ dissertation projects. Aileen has also taught health economics courses on various masters and undergraduate programs at other academic institutions (online and on-campus).
Aileen has also been a regular presenter on a training course providing an introduction to the identification, appraisal and application of economic evaluation for policy-making in public health (run by HERU in Aberdeen and funded by the Health Economics Network for Scotland).
Aileen is also the Edinburgh representative for the new Scottish Health Economics group.
The National Cancer Research Institute Annual Meeting in Glasgow 2019 marked an important milestone for members of the ECTU health economics group involved in the Lothian Cancer Data Intelligence Project (LCDI). It marked the end of an 18 month collaborative project to explore the completeness, data quality and scope of a comprehensive linked cancer regional dataset accessed by NHS Lothian Analytical Service. The project, partially funded by the Association of the British Pharmaceutical Industry, Pfizer UK, Novartis Pharmaceuticals UK Ltd, AstraZeneca UK and NHS Lothian and funded through Joint Working with Roche Products Ltd, also sought to explore the need for real world data and how to facilitate data requests from different stakeholder groups.
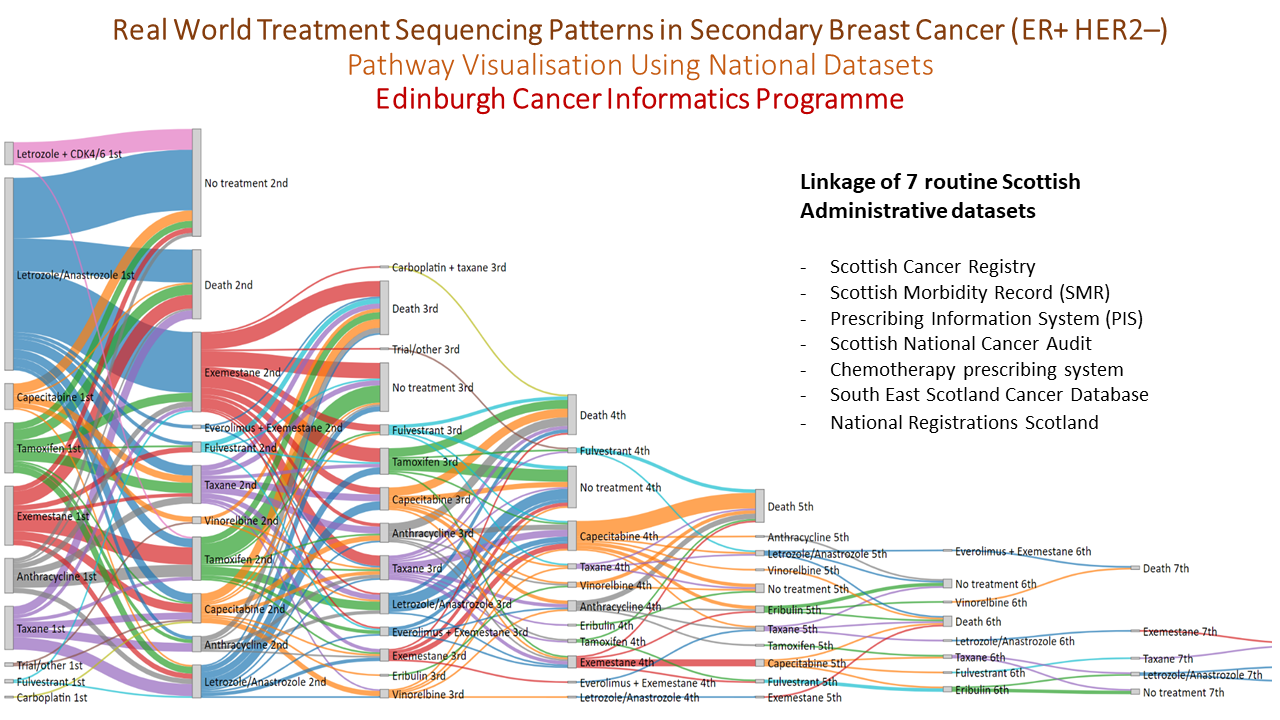
In a final meeting the key deliverables of the study were presented: a data dictionary and data quality report in the form of a wiki within the public domain and a research governance framework managed by NHS Lothian ready to pilot data requests. An important part of the project was a series of worked examples, modelled around a relevant research question, which was used to test out the processes and instructions developed as part of the LCDI study. The largest of these research questions was pathway visualisation (featured below) using national datasets to look at treatment sequencing patterns in secondary breast cancer (ER +ve HER2 –ve). This was developed into an abstract and presented at the NCRI 2019 meeting by Dr Ashley Horne as part of the Silent Theatre!
Learning from the LCDI project has led to the launch of the ‘Edinburgh Real World Data Service’ which is run jointly by the Lothian Research Safe Haven Team and the Edinburgh Cancer Informatics Programme with the objective of improving the availability and use of real NHS data to inform new reimbursement models that can ultimately provide better value medicines for NHS patients.
Learn more about the Edinburgh Real World Data Service here.
Background to the project and the think aloud pilots
The INFO-BC (Supporting shared decision making in secondary breast cancer) project is continuing to make great progress towards releasing a full-scale survey to patients, health professionals and the general public. INFO-BC is a planned survey which aims to understand preferences for secondary breast cancer treatments, you can find out more here. The study recently completed the think-aloud pilot stage of the project. 10 patients and 5 health professionals piloted early versions of the questionnaire whilst being asked to talk through their decision making. The feedback we received during the pilots allowed us to make improvements to the questionnaire, we then showed the improved version of the questionnaire to the next respondents. Changes were often made to the attributes and levels in the Discrete Choice Experiment (DCE). Attributes refer to the factors of treatment which were included in the survey and levels refer to the different available options for the attribute.
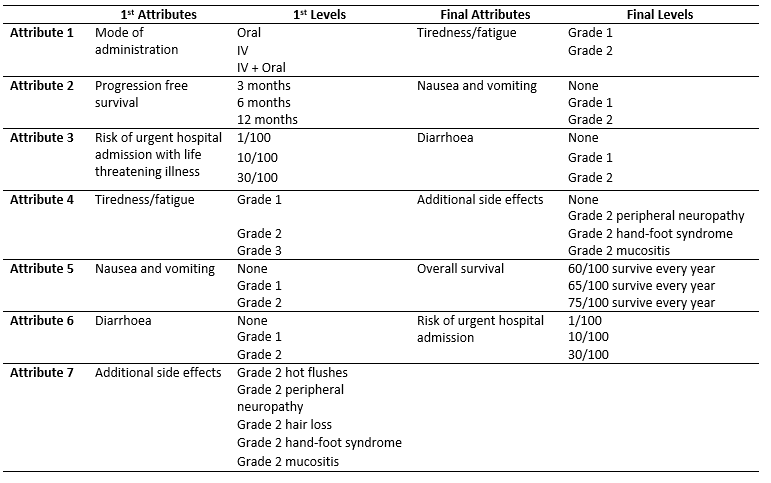
The table below illustrates how the attributes and levels changed as a result of the think-aloud pilot. Diarrhoea didn’t change significantly but you can see that it is composed of three levels; None, Grade 1 and Grade 2. Grades refer to the official Common Terminology Criteria for Adverse Events (CTCAE) which are used by health professionals worldwide to classify medical problems, symptoms, and side effects. Health professionals tend to be familiar with CTCAE criteria so were told that the grades themselves, for patients they were given a description which effectively translated the grade into standard language. There were many changes which we implanted as a result of our piloting, here I will discuss three key changes which were of particular importance.
The key changes
The first key change between the first and final version of the questionnaire was the removal of the mode of administration attribute. The decision to remove the attribute was partly because several respondents told us that the attribute was not important when compared to the other attributes. Also, we were already uncertain about whether to include the attribute, several studies similar to ours which had used a mode of administration attribute in the past found it to have little effect on people’s choices, and there is already a significant body of literature on people’s preferences for mode administration.
The second key change was that progression-free survival (PFS) was swapped for overall survival (OS). We initially failed to effectively communicate to patient respondents what PFS meant. PFS is an important measure for those who study cancer. PFS is the length of time treatment can control a cancer before it begins to grow at a clinically significant rate. It does not necessarily ensure that a patient’s life expectancy or quality of life improve. We realised that it was hard to disentangle the concepts of quality of life and length of life from patients’ interpretation of PFS. This meant that patients who chose options with better PFS weren’t necessarily interested in PFS itself, they may have been interested in a better quality of life and longer survival. A recent publication by Michael J. Raphael in Canada also came to our attention which assessed to the use of PFS in studies like ours, it argued that PFS was not being effectively communicated to patients. All of these factors considered we decided that it was simpler to ask patients to consider OS rather than PFS.
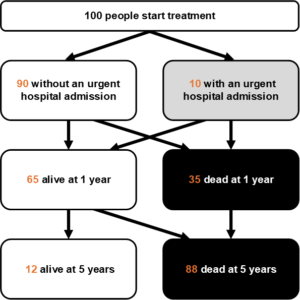
The third key change was that risk of urgent hospital admission (UHA) was combined with OS. In the early versions of the questionnaire, the respondents were shown a graphic of 100 people with some coloured in to represent risk of UHA. In a separate box, patients were shown a separate graphic illustrating the survival prospects at 1 year and 5 years for 100 people. Not only did the graphics for OS prove to be difficult to interpret but we failed to communicate to patients how the two concepts were related. In the early versions of the questionnaire, we intended the risk of UHA to be life-threatening, meaning that there was risk of death. We, therefore, attempted to communicate that the OS prospects were only relevant for individuals who completed treatment and that patients who experienced a UHA were required to stop treatment either because they had died or because treatment had proved too dangerous. This relationship was both difficult to understand and an added complication. It became apparent that we needed to more clearly and simply demonstrate the relationship. The solution we enacted was to present a single graphic as shown below which demonstrated a timeline which first showed how patients experienced a UHA within their first year of treatment, then how many patients could expect to be alive at 1 year, and how many could expect to be alive at 5 years. This solution proved to be easier to understand for respondents.
Concluding remarks
The think-aloud pilots proved to be extremely useful. I spend much time thinking about the precise scenario we are asking patients to imagine and it can be difficult to see what may be confusing to someone looking at the problem with a fresh pair of eyes. I would like to thank Morag McIntyre, the research nurse for INFO-BC, for conducting the pilots. I would also like to thank all of the patients and health professionals who took time out their days to pilot the survey and contribute to this important research.















 The group I work within focus their research on respiratory disease and the ways in which diagnosis of respiratory disease can be improved. Whilst working within this group I have been able to get fully immersed in translational research. Day to day working can involve anything from writing protocols and regulatory applications to being in the laboratory building medical devices, being in the clinics and wards assisting the clinical staff with study participants, negotiating commercial contracts for third party outsourcing, dealing with finances and creating structures and processes for forging our way through unknown territory and getting novel compounds and devices into man.
The group I work within focus their research on respiratory disease and the ways in which diagnosis of respiratory disease can be improved. Whilst working within this group I have been able to get fully immersed in translational research. Day to day working can involve anything from writing protocols and regulatory applications to being in the laboratory building medical devices, being in the clinics and wards assisting the clinical staff with study participants, negotiating commercial contracts for third party outsourcing, dealing with finances and creating structures and processes for forging our way through unknown territory and getting novel compounds and devices into man.


 Paper 2: Utilisation of personal care services in Scotland: the influence of unpaid carers
Paper 2: Utilisation of personal care services in Scotland: the influence of unpaid carers