Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
The Cardiac CARE trial tested whether tablet medications called angiotensin receptor blockers and B-blockers, taken together (cardioprotection therapy), can prevent heart muscle injury related to chemotherapy.
The health economics study question, as outlined in the Cardiac CARE protocol, is the following:
“What are the important drivers of differences in costs and quality-adjusted life-years (QALYs) between standard care and hs-cTnI-guided cardioprotection?”
The study also aims to confirm the feasibility of data capture, assess data quality and provide insight into
designing future cost-effectiveness research of hs-cTnI-guided cardioprotection.
The study found no evidence that cardioprotection therapy prevented decline in heart function in anthracycline-treated patients with elevated cardiac troponin levels and no statistically significant differences in costs and QALYs between trial arms. However, the study presented detailed tables of costs related to anthracycline therapy and cardioprotection, which could be of great use in future modelling and cost-of-illness studies.
What is the problem?
Clinical studies designed to assess the effectiveness of health technologies would ideally include outcome measures that are directly linked to utility measures of health-related quality of life. Health utilities are preference values that patients attach to their overall health status. This data is required to calculate quality-adjusted life years (QALYs) for use in cost-effectiveness analyses which is an evidence requirement for many decision makers, such as by NICE in the UK. In cases where this does not happen, an alternative solution that is extensively employed is mapping which involves using an additional data set to estimate the (statistical) relationship between outcomes measured in clinical studies and health utility.
What is Axial Spondyloarthritis?
Axial Spondyloarthritis (AxSpA) is a common rheumatic chronic progressive inflammatory disease, leading to joint damage/pain, stiffness, impaired physical function, fatigue and reductions in quality of life. The condition primarily affects the spine and sacroiliac joints. The onset is typically early in adulthood and is more common in men than in women. AxSpA patients incur significant direct NHS costs, which are mainly due to costs associated with prescriptions, and outpatient and day unit use. There are also indirect costs to society as axSpA affects young patients who have to take time off work and in the worst cases may permanently cease paid employment. The introduction of anti-TNF biologic therapies licensed for use in the management of axSpA (e.g., etanercept, adalimumab) has been associated with significantly improved outcomes. However, many of the pivotal trials for new biologics therapies did not include a generic preference-based HRQoL instrument such as the EQ-5D. Consequently, economic models of Health Technology Assessments of axSpA have been based on health utilities estimated from mapping exercises.
Our mapping study
There are no published mapping algorithms that estimate EQ-5D-5L utilities from the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) or the Bath Ankylosing Spondylitis Functional Index (BASFI) scores. We have recently had a journal article published in which we report on new mapping algorithms to obtain EQ-5D indices when only BASDAI/BASFI data are available. This is the first mapping study using a UK data set from the British Society for Rheumatology Biologics Register in AS (BSRBR-AS) which includes observations that come from England, Scotland and Wales.
What we did
Different statistical models to estimate health utility directly, or responses to individual EQ-5D questions (response mapping) indirectly from BASDAI/BASFI scores, were tested for patient self-report questionnaires. A range of metrics were used to compare and assess models performance.
Main findings
Our main study results showed that direct mapping models, and to a slightly lesser degree, response mapping models provided reliable algorithms for predicting EQ-5D-5L utilities from BASDAI/BASFI scores. These algorithms can be used in applied cost-effectiveness analysis in axSpA where EQ-5D-5L is the target outcome of interest.
A user-friendly accessible Excel tool is provided to assist analysis with the implementation of the best performing mapping algorithms (available in the online article Appendix)
The recommended mapping algorithms produced from our recent work allows researchers for the first time to estimate EQ-5D-5L values from BASDAI/BASFI data, enabling cost-utility analyses using datasets where the BASDAI/BASFI but no utility measures were collected.
The 99th Health Economics Study Group (HESG) meeting has just taken place (5-7th January 2022) at the University of Leeds. The HESG always makes for a great conference with excellent discussion and input into ongoing research. This is partly down to the unique set up of the meeting, whereby authors submit their work but they do not give a presentation of it. Instead, a discussant is assigned to read their paper and present a discussion of the research, forming a discussion agenda to encourage the audience to engage and input their thoughts and ideas.
The format truly allows for spontaneous brainstorming among the delegates and more often than not the authors leave with lots of interesting ideas, comments and suggestions to take forward in improving their work.
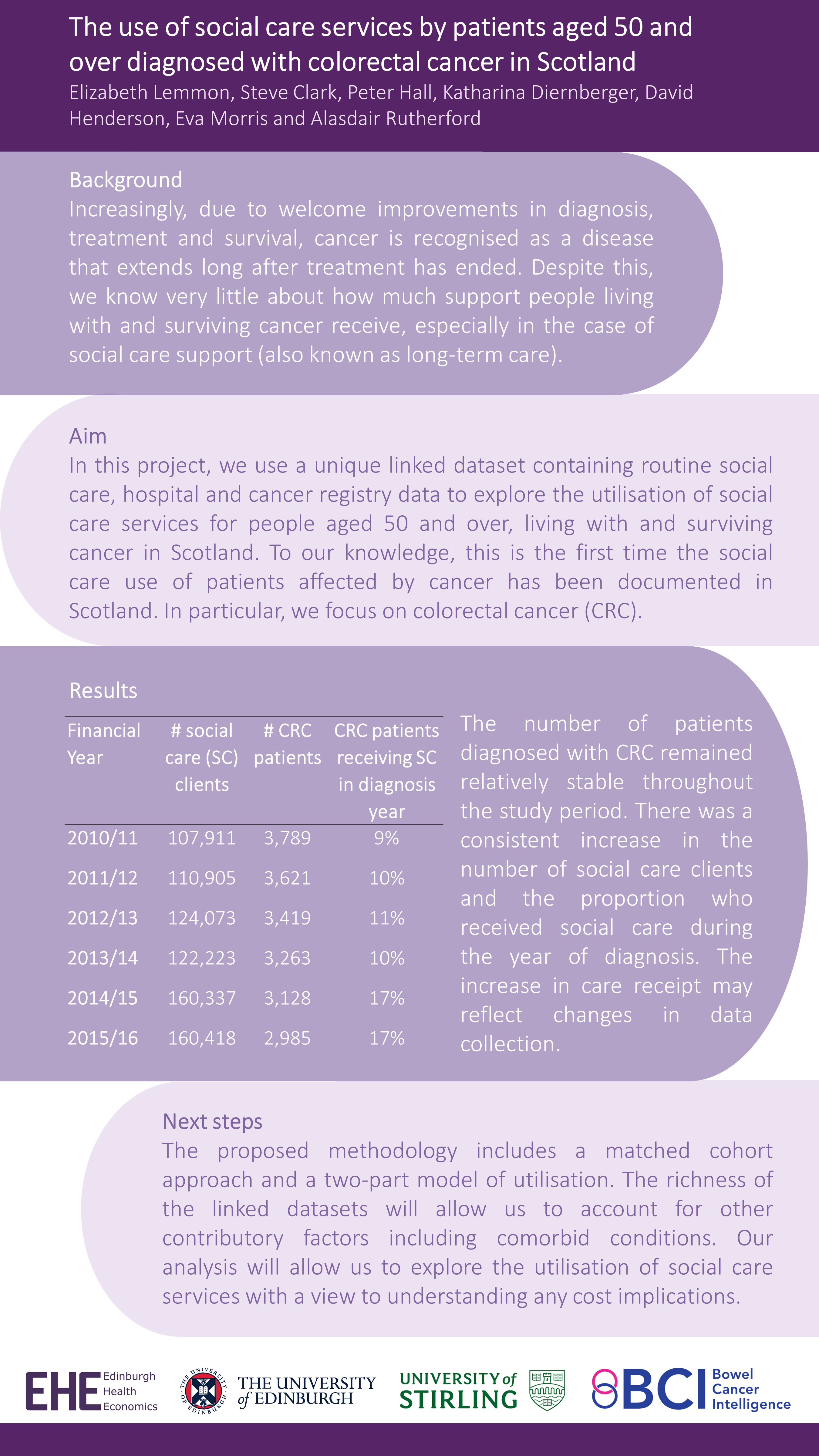
This Winter we were delighted to have our own Research Fellow, Giovanni Tramonti, representing Edinburgh Health Economics at the meeting. Giovanni was a discussant for a paper and kindly presented Elizabeth Lemmon’s et al’s work in the poster session – “The use of social care services by patients aged 50 and over diagnosed with colorectal cancer in Scotland”.
This work is the first in Scotland to analyse national data on social care service use by patients diagnosed with colorectal cancer. Check out the full poster below (all results are preliminary):
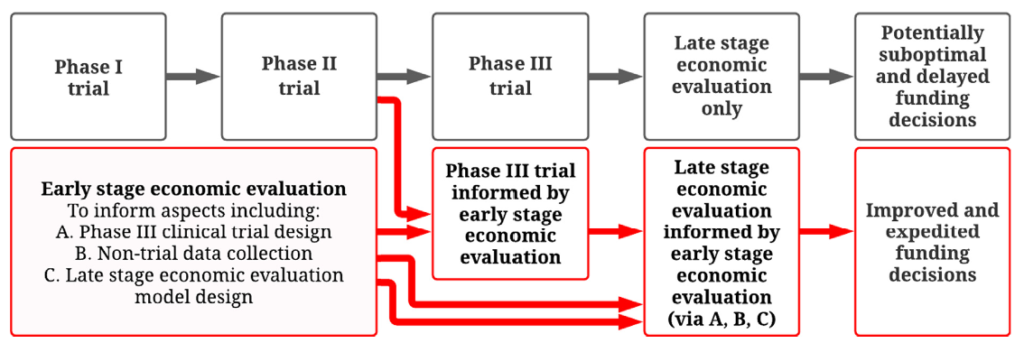
In many countries, economic evaluation is conducted using decision analytic models and must be undertaken in order to assess value for money and to make funding decisions for vaccines and other pharmaceuticals . These analyses are routinely conducted only at a late stage once the vaccine development process is complete or near complete (e.g. after phase III trials). Although economic evaluations are critical to major national funding decisions for vaccines and other drugs, there is currently no systematic planning process to meet their data requirements, which often involve many model inputs of varying uncertainty.
It is not until completion of late stage economic evaluations that we determine if the level of uncertainty in each model input is too large to reliably establish if the vaccine offers value for money. In many cases substantial uncertainty remains when reimbursement decisions are required. At this point, decision makers are faced with a dilemma. They can either recommend the vaccine based on imperfect available data and risk making a suboptimal decision (e.g. over-paying for a vaccine or not funding a vaccine that would be more beneficial than expected) or delay a reimbursement decision until more data are collected. Delays in funding vaccines can result in vaccine-preventable morbidity and mortality, while inefficient allocation of healthcare budgets can lead to less funding for other important healthcare programs.
How can early stage economic evaluation help address this problem?
Originally published December 2021 in Vaccine journal: Newall AT, Beutels P, Tuffaha HW, Hall PS, Jit M. How can early stage economic evaluation help guide research for future vaccines?
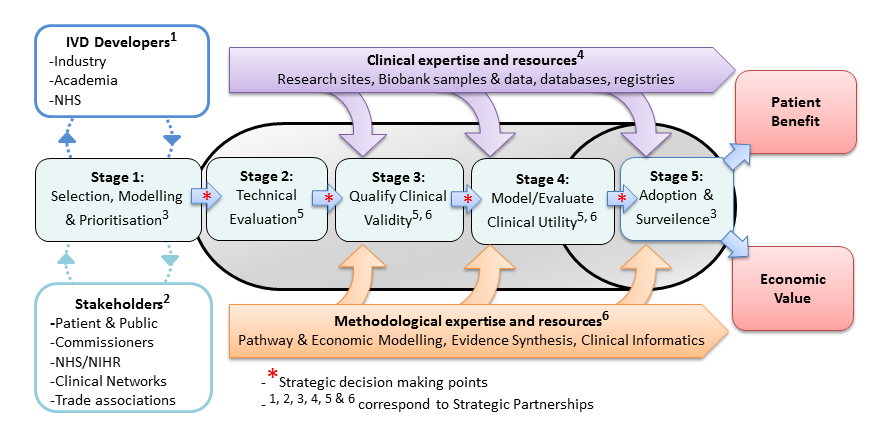
Using decision modelling and value of information analysis (VoI) early in the development of new technologies has proven an effective way of ensuring that innovation leads to high value interventions for NHS patients. There is an acute need to improve efficiency in the development of new genomic and precision medicine technologies.
With this in mind, the UK National Institute for Health Research launched four Diagnostic Evidence Co-operatives (DEC) in 2013 based at the Universities of Leeds, Newcastle, Imperial College London and Oxford. They were founded on the premise of early academic methodological engagement for programme development. A summary of their experiences in the use of early modelling is now published in the Medical Decision Making journal. Following the success of the original four DECs, the NIHR have launched an expanded network of next-generation DECs called the NIHR MedTech and In vitro diagnostic Co-operatives
Building on the earlier methodological work by Karl Claxton of the University of York and others, the Leeds DEC undertook two proof-of-concept studies led by Peter Hall to better understand the ability of early modelling, VoI and Bayesian Decision Analysis to (a) design a clinical trial of a novel diagnostic technology and (b) shape a diagnostic development portfolio for a specific disease area.
(A) The OPTIMAprelim trial used early modelling and VoI to select highest the priority genomic test from a list that included Oncotype DX, Prosigna and Endopredict, for further study in a randomised controlled trial (OPTIMA) of chemotherapy versus test-directed chemotherapy for early breast cancer.
(B) The AKI-Diagnostics project used clinical pathway modelling to understand the priorities for a UK research programme into diagnostic tests for Acute Kidney Injury in Critical Care.
Hello everyone and welcome! We are the Edinburgh Health Economics (EHE) group, part of Edinburgh Clinical Trials Unit (ECTU), and this is our new blog!
In recent years, our enthusiastic team has been growing. We now feel like it is about time that we shared with you, the research community, some of the work that we have been getting up to. For our first post, we thought that the best thing to do would be to get our Team Leader – Peter Hall – to tell you a bit about our group and our new blog.
Pete has been leading the EHE group, which bases itself within ECTU and the Usher Institute, since it was established in 2015. He is a Reader in Cancer Informatics and Health Economics, and practicing Oncologist at the Edinburgh Cancer Centre. When he isn’t treating patients, cycling to and from meetings, he is lecturing medical students, working tirelessly on one of his many research projects and keeping the EHE group on track.
Here’s what Pete had to say:
“It is an enormous privilege every day to hear the great ideas to solve problems in health economics that our group grapples with. Although Health Economists at our heart, we come from diverse backgrounds. This must be one of the reasons why we end up taking quite novel approaches to solve the established challenges of measuring value in healthcare. The environment we operate in with new data science and informatics opportunities in Scotland really gives the best opportunities to allow each of our members to shine.”
“One of our missions at the moment is to reach out to make sure that everyone knows when and how they should think about Health Economics in their research plans. The answer is ALWAYS and AS EARLY AS POSSIBLE. We hope that this blog will help you start a conversation with us. We would also love to hear from other Health Economists who share our interests.”
“As we look forward to the continuing development of EHE, the future looks bright! We hope you will join us in following this blog as we share and report on our range of activities. To find out more about our team and the projects we are working on, look out for our ‘Team Spotlight’ posts over the next few weeks!”