Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
The 99th Health Economics Study Group (HESG) meeting has just taken place (5-7th January 2022) at the University of Leeds. The HESG always makes for a great conference with excellent discussion and input into ongoing research. This is partly down to the unique set up of the meeting, whereby authors submit their work but they do not give a presentation of it. Instead, a discussant is assigned to read their paper and present a discussion of the research, forming a discussion agenda to encourage the audience to engage and input their thoughts and ideas.
The format truly allows for spontaneous brainstorming among the delegates and more often than not the authors leave with lots of interesting ideas, comments and suggestions to take forward in improving their work.
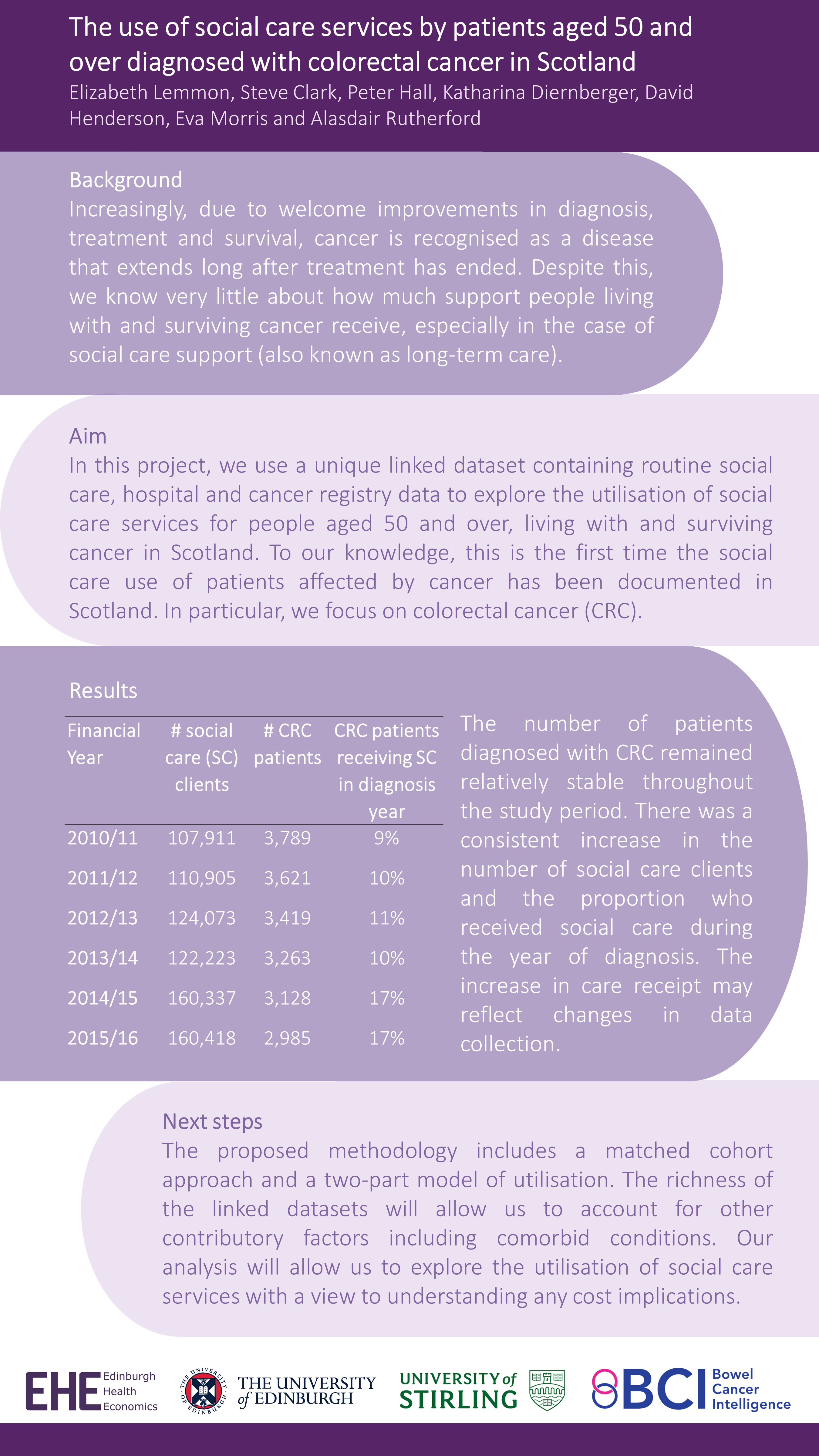
This Winter we were delighted to have our own Research Fellow, Giovanni Tramonti, representing Edinburgh Health Economics at the meeting. Giovanni was a discussant for a paper and kindly presented Elizabeth Lemmon’s et al’s work in the poster session – “The use of social care services by patients aged 50 and over diagnosed with colorectal cancer in Scotland”.
This work is the first in Scotland to analyse national data on social care service use by patients diagnosed with colorectal cancer. Check out the full poster below (all results are preliminary):
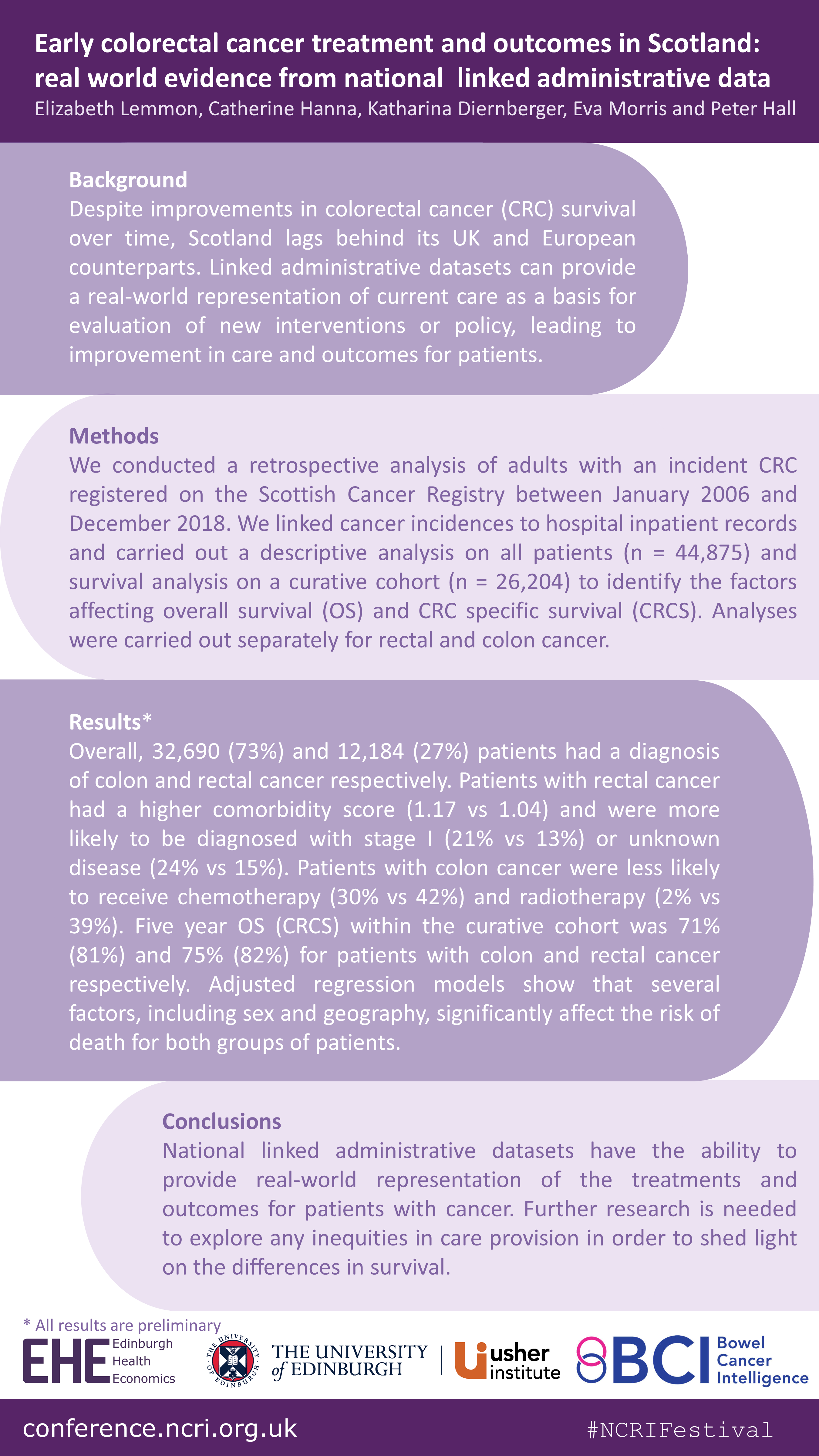
Last month (8-12 November), the Scottish Bowel Cancer Intelligence UK team at Edinburgh Health Economics attended the National Cancer Research Institute (NCRI) Festival: Making cancer research better together, with a poster on their recent work “Early colorectal cancer treatment and outcomes in Scotland: real world evidence from national linked administrative data”.
You can see more plain language summaries for the wider Bowel Cancer Intelligence programme on the BCIUK website.
Background: Whenever a patient interacts with the healthcare system, data is routinely collected, this is called “Administrative Healthcare Data”. This data can be used to provide information on screening, surveillance, existing health conditions, diagnosis, treatments and patient outcomes. It can also be used to provide information on the real-world cost of healthcare. The data is held in individual datasets, which can be linked together to provide more information than just one dataset alone.
In the UK, Administrative Healthcare Datasets are generally held separately within each nation. In Scotland, cancer data is collected by the cancer registry. This dataset contains a lot of information such as the date of diagnosis and the type and stage of cancer, but it does not include detailed information on the treatment that was delivered. In order to be able to see a full picture of what the cancer services currently look like, the cancer registry data needs to be linked to other Administrative Healthcare Datasets.
The aim of this project is to create a linked dataset to allow mapping of the bowel cancer landscape in Scotland to identify differences in the treatment offered to patients and the outcomes associated with the different treatment approaches. An additional aim is to calculate the healthcare resource needed for bowel cancer diagnosis and treatment on a national scale, and the cost of providing this.
This manuscript documents the process of creating a specific and complete bowel cancer dataset for research in Scotland.
What we did: There were four main stages in accessing and linking datasets on a national level.
Stage 1 – The first stage in accessing the data was to define the study requirements to apply to the Public Benefit and Privacy Panel (PBPP) for Health and Social Care in Scotland. The role of the PBPP is to weigh up the public benefits of granting access to healthcare data against the risks that the sharing of the data poses to an individual’s privacy.
Stage 2 – The second stage was to acquire the datasets to transfer them into the National Safe Haven (NSH). The NSH is a secure platform where the data can be used for research and analysis.
Stage 3 – All datasets that were to be released to the research team to analyse were checked by the electronic Data Research and Innovation Service (eDRIS) to make sure they matched the approved specification. The linkage of the datasets was performed by eDRIS once all the pre-checks had been completed.
Stage 4 – After the data linkages had been performed, the datasets were transferred to the National Safe Haven where researchers, with the correct approvals, could access the data. In this setting, all patient information like names and addresses were removed.
Conclusion: Linked Administrative Healthcare Datasets have huge potential to aid understanding of how patients interact with healthcare services and provide a detailed picture of the care they receive. This project demonstrates that the creation of a national linked administrative dataset is possible, by using bowel cancer data in Scotland as an example. It is however only possible through substantial effort and collaboration between researchers and the central team coordinating the data transfers and linkages.
The linked datasets have huge potential public and patient benefit by enabling researchers to analyse real world cancer data to improve outcomes for patients as well as the delivery of cancer services.
Several forces are contributing to an increase in the number of people living with and surviving colorectal cancer (CRC). However, due to the lack of available data, little is known about the implications of these forces. In recent years, the use of administrative data to inform research has been increasing. Administrative data is collected routinely ‘by government departments and other organisations for the purposes of registration, transaction and record keeping, usually during the delivery of a service’ (Woollard, 2014). Examples include hospital admissions data, education records and tax records.
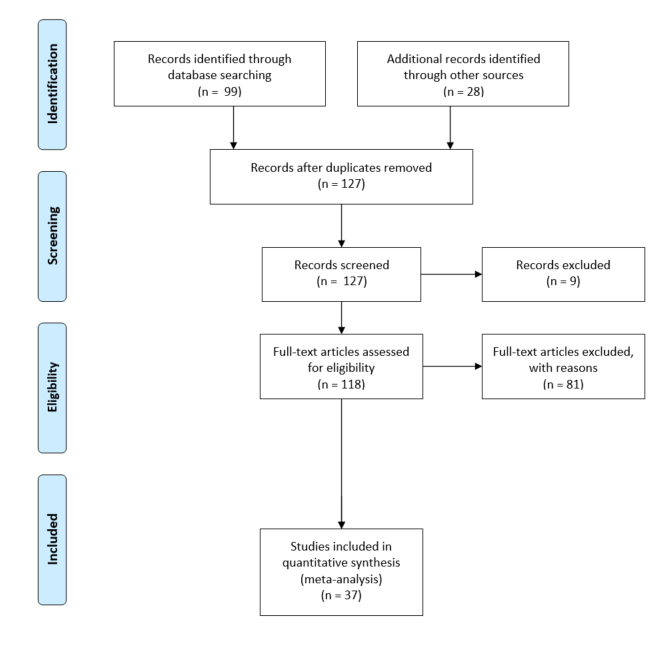
The aim of one of our recent pieces of work was to investigate the potential contribution that this type of data could have on the health economic research of CRC. To achieve this aim, we conducted a systematic review of the health economic CRC literature published in the United Kingdom and Europe within the last decade (2009– 2019).
Our specific objectives were:
To summarise the existing health economic research of CRC in the UK and Europe;
To identify whether and what types of administrative data were used within this research;
To explore the benefits and limitations of using administrative data in this research;
To discuss the ways in which administrative data, using Scotland as an exemplar, could contribute to this research in the future
The literature search identified thirty- seven relevant studies, which we divided into economic evaluations, cost of illness studies and cost consequence analyses.
Findings:
We found that the use of administrative data, including cancer registry, screening and hospital records, within the health economic research of CRC is commonplace. However, we found that this data often come from regional databases, which reduces the generalisability of results.
Further, we found that administrative data appear less able to contribute towards understanding the wider and indirect costs associated with the disease, particularly with respect to social care and indirect costs such as unpaid care.
We also found that very few papers adopted a societal perspective when carrying out their evaluation meaning that often only direct medical care costs were included.
Finally, we found that administrative data were less able to contribute when it comes to measuring patient health related quality of life (HRQoL) and preferences for those health states, which is vital particularly in EEs.
We explore several ways in which various sources of administrative data could enhance future research in this area. If you want to find out more, head on over to the European Journal of Cancer Care website where you can read the article in full.
At the end of April, Peter and Elizabeth, along with lead author Dr Catherine Hanna and patient representative Mr Steve Clark, presented their recent publication at the Power of Population Data Science Webinar Series.
Lucky for you, if you missed the webinar, you can watch it again on the Population Data BC YouTube channel here and see our slides from the event here.
The webinar was very well received with over 111 people signed up to the event and around 70 in attendance on the day. We were thrilled to spread the word about all of the hard work that has gone into creating this dataset, as well as all of the research we have planned so watch this space!
This summer, after running our first undergraduate Health Economics module, a couple of enthusiastic economics students approached us to ask if there were any opportunities to get some work experience with Edinburgh Health Economics. Whilst we don’t run any formal internship schemes, we thought we could definitely think of some useful projects for the students to get involved with. In this post, one of those students talks to us about the work that she did during her voluntary internship and offers some reflections on how she found the experience overall.
Intern profile
Name: Emma Wilson
Bio:“I recently graduated (virtually!) in Economics from the University of Edinburgh in July 2020 and I am currently working as a Competition Economist for the Financial Conduct Authority. I have had a strong interest in Health Economics since I started working for the NHS in the first year of university in the holidays, and I then took the Health Economics course in fourth year solidifying my interest. My interest resulted in me writing a health/labour market dissertation about gender differences in wages due to health.”
Internship activities
“During my internship I have been working on part of the CORECT-R project. The project aims to create a UK wide Colorectal Cancer Intelligence Hub and identify the opportunities to impact on care to improve outcomes across the UK and provide evidence to guide interventions that will minimise inequalities and improve survival. I have specifically been working with Dr Elizabeth Lemmon on a report on costing methodology heterogeneity called ‘Validating costing methodologies used in the health economic literature of colorectal cancer’. You can view the report here.
The report looks at a cross-section of 20 papers of the most recent health economics literature on colorectal cancer. The studies are compared and contrasted against not only one another, but also against costing methodology criteria that has been laid out in a previous study on costing in health economics. It is concluded that due to ambiguity around costing methodologies and I suggest several ways in which the transparency around costing can be improved: studies should explicitly state whether they use micro, gross, top-down or bottom-up costing, providing clear evidence of how they do so; studies should also provide clarity in their computations and clearly state cost sources, and the identification process of costs used should be made clear. I suggest at the end of my report that a CHEERS type checklist for costing should be created in the future to ensure that costing methodologies are more homogeneous and allow for studies to be easily replicated and generalised.”
Intern reflections
“During my internship my critical literature analysis skill have increased hugely from examining a large number of academic papers and examining them. My academic writing skills have also improved from the constant feedback loop I have had with Dr Lemmon. The autonomy that I have been given to work on the project has been something I have never had before, and I have enjoyed the accountability I have been able to take for my work. The internship has been a great opportunity, and I would highly recommend it to anyone else with an interest in health economics, or in improving their analysis or academic skills.”
Project lead reflections
“From our perspective, it was brilliant to have Emma on board to help with the costing methodologies used within the health economics literature on colorectal cancer. This is an area in which we have found significant heterogeneity and Emma’s work confirms and documents this. Her work will be extremely helpful for the project going forward. Overall, Emma was a pleasure to work with and she has really set the bar for future ‘interns’!” Elizabeth Lemmon