Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
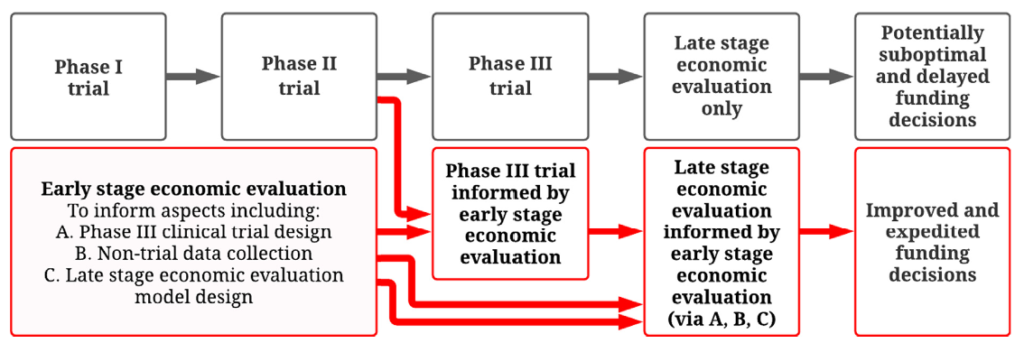
In many countries, economic evaluation is conducted using decision analytic models and must be undertaken in order to assess value for money and to make funding decisions for vaccines and other pharmaceuticals . These analyses are routinely conducted only at a late stage once the vaccine development process is complete or near complete (e.g. after phase III trials). Although economic evaluations are critical to major national funding decisions for vaccines and other drugs, there is currently no systematic planning process to meet their data requirements, which often involve many model inputs of varying uncertainty.
It is not until completion of late stage economic evaluations that we determine if the level of uncertainty in each model input is too large to reliably establish if the vaccine offers value for money. In many cases substantial uncertainty remains when reimbursement decisions are required. At this point, decision makers are faced with a dilemma. They can either recommend the vaccine based on imperfect available data and risk making a suboptimal decision (e.g. over-paying for a vaccine or not funding a vaccine that would be more beneficial than expected) or delay a reimbursement decision until more data are collected. Delays in funding vaccines can result in vaccine-preventable morbidity and mortality, while inefficient allocation of healthcare budgets can lead to less funding for other important healthcare programs.
How can early stage economic evaluation help address this problem?
Originally published December 2021 in Vaccine journal: Newall AT, Beutels P, Tuffaha HW, Hall PS, Jit M. How can early stage economic evaluation help guide research for future vaccines?
For any queries please contact Lesley Innes (she@abdn.ac.uk)
SHE was launched in 2019 to support, promote and further develop health economics in Scotland. SHE is a collaboration of health economists from Scotland’s Universities, NHS and Government. Our aim is to bring together researchers and users of health economics to explore the development and application of health economics in Scotland.
Although there have been substantial developments in the analysis of uncertainty in economic evaluations of health care programmes, the development of methods for one-way sensitivity analysis has been notably slower.
Conditional incremental net benefit was recently proposed as an approach for implementing probabilistic one-way sensitivity analysis for economic evaluations comparing two strategies.
Here, we generalise this approach to economic evaluations that compare three or more strategies.
We find that ‘conditional net benefit’ may be used to conduct probabilistic one-way sensitivity analysis for economic evaluations comparing any number of strategies.
We also propose the ‘conditional net benefit frontier’, which may be used to identify the most cost-effective of any number of strategies conditional upon the specific value of a parameter of interest.
We are conducting a study to get a better understanding of what is important to secondary breast cancer patients when making treatment decisions. We are also looking at what is important to the clinical team looking after the patients and to the general public. Our study aims to support shared decision making between patients and clinicians. The project is called the INFO-BC study. Read more on the HERU blog bit.ly/37n3ZB9
People who are nearing the end of life are high users of hospital services. The absolute cost to providers and its value is uncertain. There is a need to identify which groups of people spend a lot of time in hospital so that care can be modified to better tailor care to patients preferences and to improve the efficiency health services in this context.
Research Summary
Objectives: To describe the pattern, trajectory and drivers of secondary care use and cost by people in Scotland in their last year of life. Methods: Retrospective whole-population secondary care administrative data linkage study of Scottish decedents of 60 years and over between 2012 and 2017 (N=274,048).
Results: Secondary care use was high in the last year of life with a sharp rise in inpatient admissions in the last three months. The mean cost was 10,000 pound. Cause of death was associated with differing patterns of healthcare use: dying of cancer was preceded by the greatest number of hospital admissions and dementia the least. Greater age was associated with lower admission rates and cost. There was higher resource use in the urban areas. No difference was observed by deprivation.
Conclusions:
Hospitalisation near the end of life was least frequent for older people and those living rurally, although length of stay for both groups, when they were admitted, was longer.
Research is required to understand if variation in hospitalisation is due to variation in the quantity or quality of end of life care available, varying community support, patient preferences or an inevitable consequence of disease-specific needs.
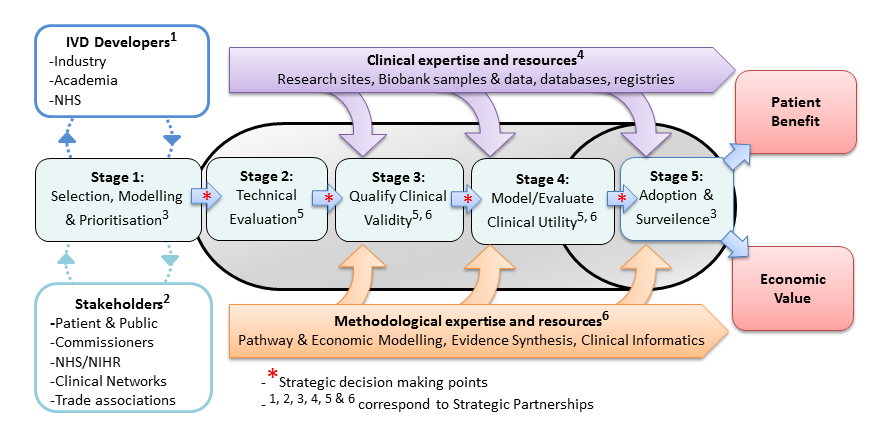
Using decision modelling and value of information analysis (VoI) early in the development of new technologies has proven an effective way of ensuring that innovation leads to high value interventions for NHS patients. There is an acute need to improve efficiency in the development of new genomic and precision medicine technologies.
With this in mind, the UK National Institute for Health Research launched four Diagnostic Evidence Co-operatives (DEC) in 2013 based at the Universities of Leeds, Newcastle, Imperial College London and Oxford. They were founded on the premise of early academic methodological engagement for programme development. A summary of their experiences in the use of early modelling is now published in the Medical Decision Making journal. Following the success of the original four DECs, the NIHR have launched an expanded network of next-generation DECs called the NIHR MedTech and In vitro diagnostic Co-operatives
Building on the earlier methodological work by Karl Claxton of the University of York and others, the Leeds DEC undertook two proof-of-concept studies led by Peter Hall to better understand the ability of early modelling, VoI and Bayesian Decision Analysis to (a) design a clinical trial of a novel diagnostic technology and (b) shape a diagnostic development portfolio for a specific disease area.
(A) The OPTIMAprelim trial used early modelling and VoI to select highest the priority genomic test from a list that included Oncotype DX, Prosigna and Endopredict, for further study in a randomised controlled trial (OPTIMA) of chemotherapy versus test-directed chemotherapy for early breast cancer.
(B) The AKI-Diagnostics project used clinical pathway modelling to understand the priorities for a UK research programme into diagnostic tests for Acute Kidney Injury in Critical Care.
“For my master’s dissertation, I was beyond excited to get involved in a real-life health economics project at the Edinburgh Clinical Trials Unit”
Population aging is a worldwide phenomenon, projecting a rise in the number of persons aged over 60 from approximately 810 million currently, to 2 billion by 2050 (O’Brien, 2013). The observed rise in longevity is a major public health achievement which reflects advances in medicine, healthcare, sanitation, nutrition, education and the economy. However, it also poses numerous novel challenges for future provision of health and social care, as the prevalence of life-limiting illnesses, disabilities, and comorbidities rise with the aging population. The ageing population is one of many public health challenges, urging innovators, researchers, politicians, and doctors alike to brainstorm creative solutions. The idea of connecting the dots between myriad of aspects which influence health in our society to make an impact at the level of population urged me to further my studies in public health at the University of Edinburgh. However, as the first week of orientation progressed, information overload on the wide-ranging fields within public health including ethics, epidemiology, health promotion, health policies, health technology assessment, health security—and the list goes on—left me feeling more confused than before. I felt lost and had no idea which direction I should take my studies in the short year I had in Edinburgh.
Shortly after, I found clarity when I was introduced to health economics and its fascinating nature. I was instantly drawn to the unique qualities of healthcare as a commodity and its influence on delivery. I thought to myself, why is it so difficult to get the healthcare system right? It seems to be one of those issues that everyone has an issue with. No one country’s healthcare system keeps everyone satisfied. The US has its problems of insurance coverage and the NHS has long suffered from excessive waiting time due to shortage of supply and increasing demand. Health economics is intimately intertwined with this problem, and for me, it brought into light the highly contested debate amongst health policy makers concerning the method of healthcare delivery, and whether market forces better allocate resources compared to the state (Mwachofi and Al-Assaf, 2011). A common position held in healthcare reform is that the state should not interfere and allow the natural market forces to allocate resources efficiently (ibid). However, the argument is constructed on a supposition that the healthcare fulfils all the conditions necessary for a perfect market, which is far from the truth. One of many exceptions is imperfect knowledge of consumers which necessitates for healthcare professionals to provide expert advice on formulating healthcare consumption decisions (Morris et al., 2012). However, the same healthcare professionals such as doctors, are also the supplier of the healthcare goods, hence are able to influence the demand. This existence of information asymmetry and physician-induced demand puts physicians in a position of power over their patients thus regulations become necessary. When the overall objective of healthcare system is efficiency as well as equity, interventions from an interdisciplinary team including the government, economists, physicians, policy makers and alike, are essential. Further, with the emergence of numerous public health challenges and limited resources, it is imperative that every decision being made is serving the goals of equity and efficiency.
For my master’s dissertation, I was beyond excited to get involved in a real-life health economics project at the Edinburgh Clinical Trials Unit. I got an opportunity to practice what I learned in the classroom toward practical application on the effective allocation of resources and the challenge of aging population and palliative care. My dissertation was a feasibility study to evaluate the economic impact of a new and coming Exercise and Nutrition-based Rehabilitation (ENeRGy) programme for patients with advanced cancer undergoing palliative care. The development of such programme is a result of the recent shift in attitude toward end-of-life care which acknowledges the importance of timely and early intervention. Specialist palliative care teams and multi-professional approaches have shown to improve health outcomes and effect cost by reducing the amount of time patients spend in acute hospital inpatient environment and out-of-home services (Gaertner et al., 2015). Increasing evidence supports the concept of early and specialised palliative care, however the implementation of sustainable interventions depends on the means for pragmatic matters such as resource allocation and funding. Hence, I worked with data from the ENeRGy trial to compare and contrast the cost of healthcare resource utilisation between patients in the control and intervention groups. As well, I had the opportunity to assess the quality of the evidence related to successful implementation and the validity of the method for cost ascertainment for future trials, specific to the UK Cancer Cost Questionnaire developed by the ECTU.
Throughout the long 3 months of tackling this feasibility project, I encountered many challenges. From scrambling to convince the non-intuitive parts of my brain to figure out how to write codes in order to do statistical analysis—to endless error scripts testing my patience and perseverance. Moreover, in many instances, I had to battle feelings of doubt in my methods and results as I attempted to fill my dissertation from a blank page. In particular, I was struck by the lack of homogeneity and standardised methods in assessing healthcare utilisation in palliative care. Methodologies in the UK varied especially, due to the complex public funding systems and the NHS. Hence, health economists have to resort to the convoluted documents of national tariffs and ‘Unit Costs of Health and Social Care’ which attempt to make estimates on each health care services. I also found the sense of emotional disconnect between working with ‘data’ which represent real patients and families burdened by advanced cancer, quite perplexing.
I found from both the literature review and secondary data analysis that the use of community-based healthcare services could shift the burden from costly hospital-based services to community services thereby leading to cost-savings. Ultimately the results of the cost-analysis indicated that the implementation of the ENeRgy program has the potential to drive significant cost-savings in palliative care for patients with advanced cancer. On a personal level, I acquired a deeper appreciation for health economics and the multi-faceted nature of the field. Although, it could be easy to feel disconnected from reality as we work with just numbers, and data, health economics—I realised is much more, encompassing aspects of ethics, governance, and stands as a powerful tool to achieve milestones in public health, by strengthening health systems. For example, as we strive towards universal health coverage across the globe, it is essential to have equity in access to health services, as well as ensure affordability of services, which are both central to health economics (WHO, 2019). As I move onto the next steps, I am grateful to have had this experience and acquired the skills to continue in the field of healthcare and research.
References
Gaertner, J., Maier, B.-O. and Radbruch, L. (2015). Resource allocation issues concerning early palliative care. Annals of Palliative Medicine, 4 (3), 156-161–161.
Morris, S. et al., (2012). Economic analysis in health care Second., Chichester: Wiley.
Mwachofi, A., & Al-Assaf, A. F. 2011. Health care market deviations from the ideal market. Sultan Qaboos University medical journal, 11(3), 328-37.
O’Brien, T. (2013). The Impact of an Aging Population on Palliative Care. Journal of Pain & Palliative Care Pharmacotherapy, 27 (4), 389–391.