Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
The 99th Health Economics Study Group (HESG) meeting has just taken place (5-7th January 2022) at the University of Leeds. The HESG always makes for a great conference with excellent discussion and input into ongoing research. This is partly down to the unique set up of the meeting, whereby authors submit their work but they do not give a presentation of it. Instead, a discussant is assigned to read their paper and present a discussion of the research, forming a discussion agenda to encourage the audience to engage and input their thoughts and ideas.
The format truly allows for spontaneous brainstorming among the delegates and more often than not the authors leave with lots of interesting ideas, comments and suggestions to take forward in improving their work.
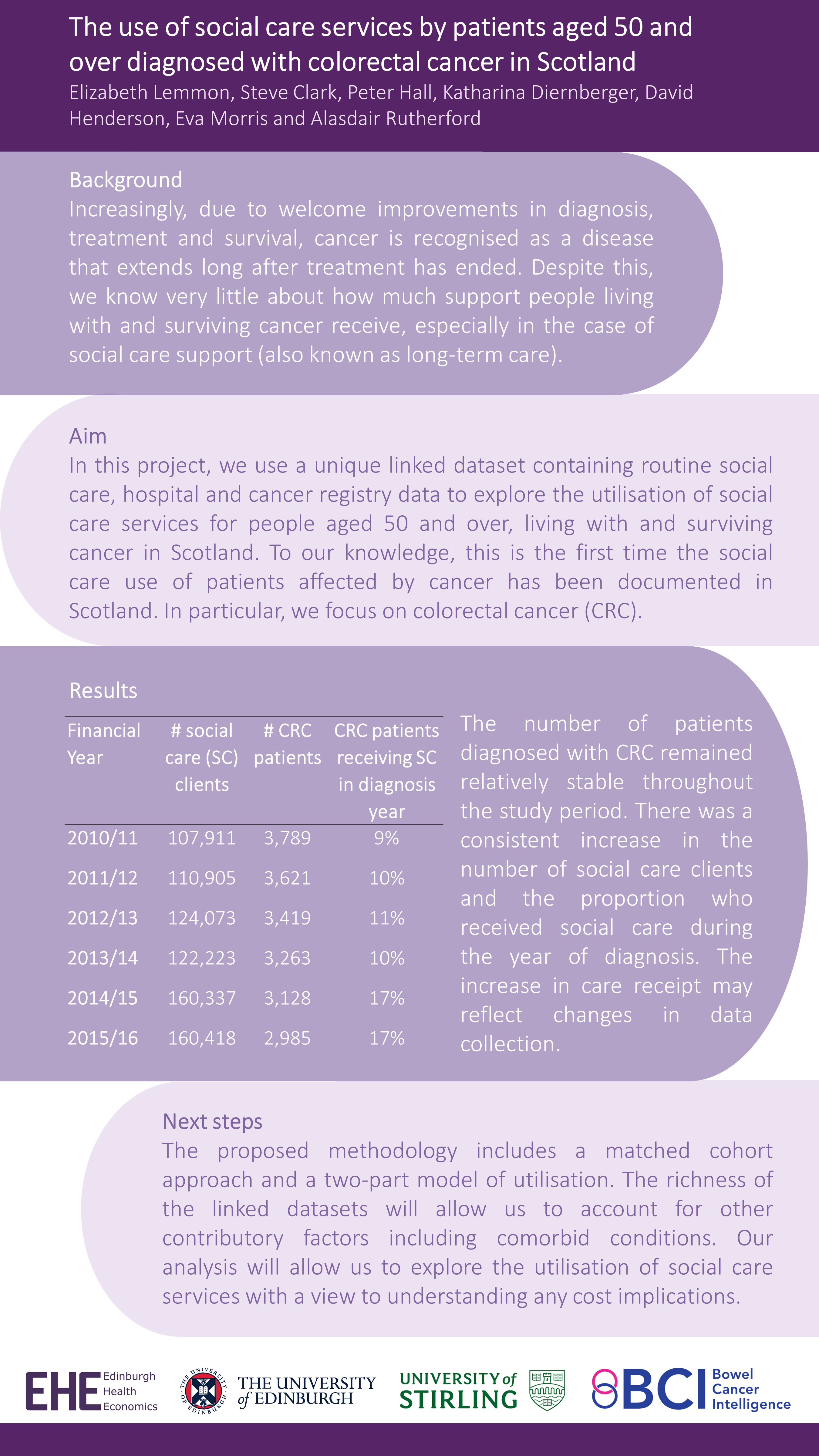
This Winter we were delighted to have our own Research Fellow, Giovanni Tramonti, representing Edinburgh Health Economics at the meeting. Giovanni was a discussant for a paper and kindly presented Elizabeth Lemmon’s et al’s work in the poster session – “The use of social care services by patients aged 50 and over diagnosed with colorectal cancer in Scotland”.
This work is the first in Scotland to analyse national data on social care service use by patients diagnosed with colorectal cancer. Check out the full poster below (all results are preliminary):
Health Economics Study Group and Discrete Choice Experiments
I am the primary researcher on INFO-BC. We plan to implement a discrete choice experiment (DCE). A DCE is a type of stated preference exercise where respondents make decisions hypothetical scenarios. Our team identified opportunity to use DCE’s in a secondary breast cancer setting. At the start of July I attended the Summer Health Economics Study Group (HESG) at the University of East Anglia (UEA), needless to say one of my main objectives was to discover what my peers in other parts of the UK doing in the area of preference elicitation. I found the three studies particularly interesting and have provided a summary of each of them here:
Moffatt. P, King. M, Viney. R, White. B, Butler. L, 2019. Impact and detection of straightlining response in health surveys (working paper)
The problem of straightlining is prominent in DCEs. Straightlining is when a respondent does not engage in a DCE and is instead found to be consistently choosing at random or choosing according to arbitrary factors, such as always choosing the option on the left. The authors demonstrated the problem of straightlining in an example DCE. They also propose methods to identify straightliners and mitigate the problem. The proportion of straigliners identified was high at 45.2%, although there were concerns from the audience that the DCE used in the study was particularly complex and was therefore likely to have a higher proportion of straighliners. The methods which excluded individuals identified as straightliners appeared to provide more reliable estimates, although it remains to be seen if the same method would have the same results in the case of a more typical DCE design where there is likely to be a smaller proportion of straightliners.
McNamara. S, Tsuchiya, A. Holmes, J, 2019. Which preferences? choice architecture and normative health economics (working paper)
Stated preference exercises all have a choice architecture which affects how respondents interpret information and the decisions they make. This in turn impacts the resulting preferences. In health economics the results of stated preference can have real world effects on the decisions to provide or not provide treatments and technologies. In this study the authors illustrate how choice architecture can affect preferences using the example of a stated preference exercise eliciting public aversion to health inequalities. The authors address three key questions.
If preferences are architecture sensitive, should we be using them in health-economic evaluation?
If preferences are to be used in this way, what type of preference should we be using?
How should we be structuring choice architectural decisions?
In summary the authors argue for the use of preferences assuming the approach is reasonable. They propose four questions to help Heath Economists structure their choice architecture. Finally they call for closer collaboration of Health Economists, behavioural scientists, philosophers, and policy makers to address the issue the sensitivity of preferences for choice architecture.
Boyers. D, Van der pol. M, Watson. V, 2019. The impact of ex-ante correction methods on hypothetical bias in Discrete Choice Experiment responses: A case study in dental care (working paper)
I acted as the discussant for this paper. The authors experimented with methods designed to mitigate hypothetical bias from their DCE. Hypothetical bias specifically refers to bias that arises when respondents fail to respond to a DCE in the same way that they would respond in an equivalent real life scenario. There was some evidence that two interventions went a small part of the way to mitigate hypothetical bias, these interventions were an honesty oath and a consequentiality script. To simplify the interventions: the honesty oath asked respondents to tick a box before the experiment and thereby promise to give honest responses; the consequentiality script informed respondents of the consequences the DCE is likely to have on policy decisions. The honesty oath was accompanied with the added complication that the completion rate was 10.3% lower than the baseline. The general verdict of the myself audience was that this is an interesting area for further research but that one would have reservations about implementing the proposed interventions unless stronger evidence was produced.