

In this extra post, Avita Rath builds on existing scholarship on teacher noticing and noticing in health professions education, while extending the discussion to clinical educator practice in dental education and resource-constrained teaching contexts. The post speaks broadly to learning and teaching, clinical education, professional identity formation, feedback, and staff development in teaching practice. Avita is an alumni of the MSc Clinical Education at Edinburgh Medical School, and currently a dental educator based in Malaysia.
Clinical teaching often appears, from the outside, to be about explaining, demonstrating, supervising and assessing. Yet much of its most important work begins before any of these visible acts. It begins with noticing.
A clinical educator notices the student who can recite the theory but hesitates when holding the instrument. The patient whose discomfort is not yet verbalised. The learner who nods politely while still feeling lost. The student who appears confident, but is not yet safe. The moment when correction is necessary, but must be offered without shame.
In these small acts of attention, clinical teaching becomes more than the transmission of knowledge. It becomes a practice of judgement, care and safety.
Noticing differently in clinical education
Noticing is not new. It has been examined in teacher education as a way teachers attend to and interpret classroom situations (König et al., 2022), and more recently in health professions education as a capacity that may need to be cultivated deliberately in learning and practice (Clement et al., 2023).
What I want to ask is slightly different: what does the clinical educator notice while holding together student learning, patient safety, professional formation and care — often all at once?
This question feels especially live in dental education, where learning happens in close proximity to patients, instruments, time pressures and embodied skill. In my own clinical teaching, I have often found that what matters most is not always the most dramatic error, but the small hesitation, the altered grip, the patient’s expression, or the student’s pause before asking for help.
Four sites of clinical noticing
I have begun to think of clinical educator noticing through four sites (Figure 1): the hand; the face; the threshold; and the becoming clinician. These are not separate checklists to attend to in a specific order, but overlapping moments of attention in the clinic.
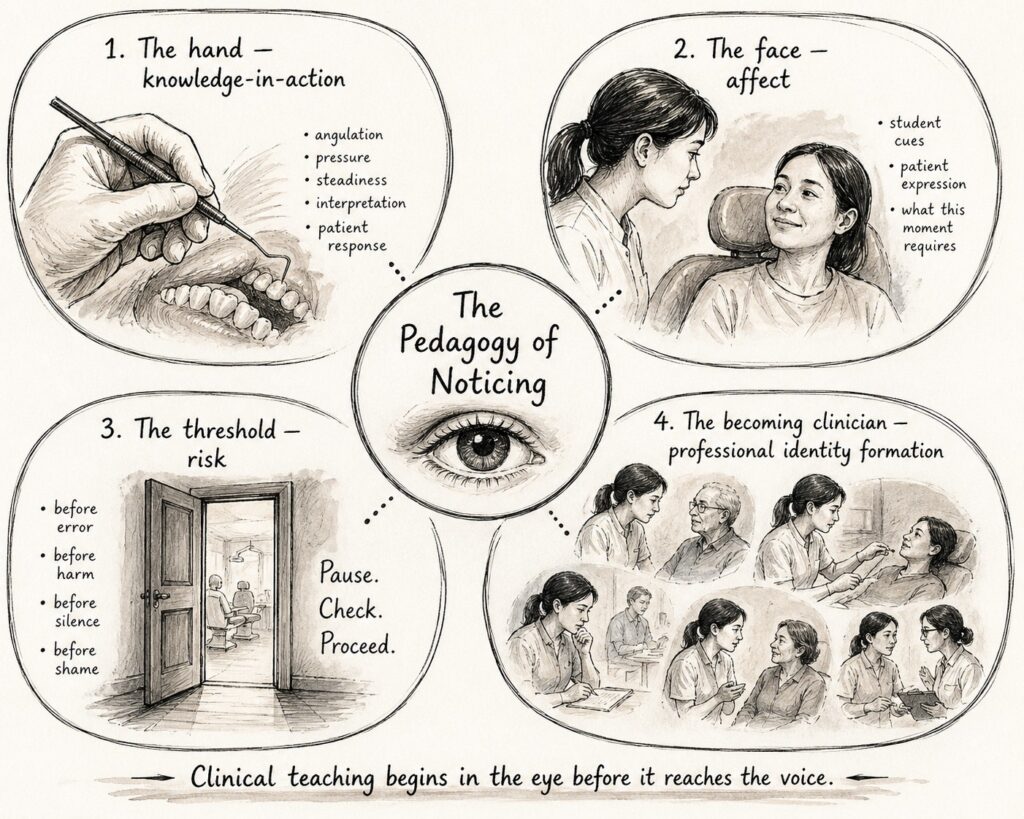
1. The hand: noticing knowledge-in-action
A student may describe periodontal probing accurately, yet the educator notices whether knowledge is carried into the body — the angulation of the probe, the steadiness of the hand, the interpretation behind each movement, and the patient’s response to pressure or discomfort. This resonates with Goodwin’s idea of “professional vision”: the ways professionals learn to see what matters within a specific field of practice (Goodwin, 1994).
2. The face: noticing affect
Students do not always tell us when they are anxious or overwhelmed. Sometimes they smile. Sometimes they overcompensate with confidence. Sometimes the patient’s face tells us what the student has missed. We learn to read these small signs — not to psychoanalyse, but to decide what this moment requires: correction, reassurance, space, challenge, or simply a pause. This reading is itself a kind of emotional work, often unnamed in the formal curriculum and unevenly distributed across those who teach.
3. The threshold: noticing risk
Clinical learning is full of thresholds: before a mistake becomes harm; before uncertainty becomes silence; before confidence becomes unsafe; before feedback becomes humiliation. The educator notices when a student is about to compromise comfort, consent, infection control or professionalism — often before the mistake becomes visible to others. This is quiet, preventive work.
4. The becoming clinician: noticing professional formation
We also glimpse who students are becoming: how they speak to patients; whether they take responsibility; whether they pause; whether they ask for help. Professional identity is not formed in lectures alone. It is shaped in repeated clinical encounters, under observation, pressure and care.
Why this matters in stretched contexts
Working in a Malaysian private university has made me particularly attentive to the conditions under which noticing happens. Clinical educators often teach within uneven resources, diverse student preparedness, multilingual realities and limited time. These conditions are not only deficits; they shape a particular pedagogical intelligence. Practices of noticing can support teaching in these conditions:
- When time is short, noticing helps us prioritise.
- When students are diverse, noticing helps us individualise.
- When systems are stretched, noticing helps us protect what matters.
Yet this work is rarely named. It can look like instinct, personality, or simply ‘good teaching’. If we leave noticing unnamed, we leave it unsupported — and we leave novice educators to assume that experienced teachers simply ‘see more’, without understanding how such seeing is built through practice, mistakes, mentorship and dialogue. Research on teacher noticing suggests that noticing can be conceptualised, studied and developed, rather than treated as a vague personal quality (König et al., 2022; Weyers et al., 2023).
Can noticing be taught?
I think it can — but perhaps not through checklists alone.
We can teach noticing by talking openly about what we see in clinical encounters and why it matters. We can invite junior colleagues to observe not only what we say to students, but when we choose to intervene, wait, redirect or remain silent. Post-clinic debriefs can ask:
- What did you notice?
- What did you miss?
- What made you step in?
- What did the student need?
- What did the patient need?
We can also encourage students to develop their own noticing — of patient cues, uncertainty, their own assumptions, and the difference between completing a procedure and caring for a person. Recent work in health professions education has begun to explore how noticing might be intentionally cultivated with learners rather than left to chance (Clement et al., 2024).
For me, this is where clinical teaching becomes deeply pedagogical. Noticing is care before action, judgement before feedback, safety before assessment. Perhaps one task of faculty development is not only to help educators give better feedback, but to recognise the attentive work that happens before feedback is even spoken.
Clinical teaching begins in the eye before it reaches the voice.
References
Clement T, Bolton J, Griffiths L, Cracknell C, Molloy E. ‘Noticing’ in health professions education: Time to pay attention? Medical Education. 2023;57(4):305–314. doi:10.1111/medu.14978.
Clement T, Denniston C, Cracknell C, Bolton J, Norris N, Molloy E, Donald KJ, Virtue D, Tey C. Towards a pedagogy for noticing: Piloting a novel intervention for health professions students. Medical Teacher. 2024;46(11):1407–1409. doi:10.1080/0142159X.2024.2353735.
Goodwin C. Professional vision. American Anthropologist. 1994;96(3):606–633. doi:10.1525/aa.1994.96.3.02a00100.
König J, Santagata R, Scheiner T, Adleff AK, Yang X, Kaiser G. Teacher noticing: A systematic literature review of conceptualizations, research designs, and findings on learning to notice. Educational Research Review. 2022;36:100453. doi:10.1016/j.edurev.2022.100453.
Weyers J, König J, Santagata R, Scheiner T, Kaiser G. Measuring teacher noticing: A scoping review of standardized instruments. Teaching and Teacher Education. 2023;122:103970. doi:10.1016/j.tate.2022.103970.
 Avita Rath
Avita Rath
Dr Avita Rath is a dental educator based in Malaysia and an alumna of the MSc Clinical Education programme at the University of Edinburgh. Her teaching and research interests include health professions education, emotional labour, clinical teaching, professional identity formation, feedback, and equity in resource-constrained educational contexts.
