Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
In May 2025 the Suicide Cultures project hosted a 2 day symposium focused on the sociology of suicide. This is a topic that is central to the project, given our own aims to grow sociological research on suicide, as well as to showcase and share how sociological expertise and research can transform how suicide is studied and responded to in policy and practice.
The symposium featured a number of current and former researchers who have contributed to Suicide Cultures. They were joined by a range of additional speakers, each sharing different sociologically informed research addressing suicide. Two of our Advisory Board members – Professors Anna Mueller and Seth Abrutyn – joined us as well, providing an excellent plenary discussion, as well as giving a public lecture at the end of the seminar. The recording of the lecture, which centred on Anna and Seth’s latest book, Life Under Pressure, can be accessed here.
The symposium was free to attend, and we welcomed 45 attendees across the two days, including researchers, PhD students, people with lived/living experiences of suicide, policy makers and practitioners.
The full programme of the symposium can be viewed below, which gives a flavour of some of the exciting and engaging talks and discussions that the symposium enabled.
The two days were organised around panel presentations, as well as roundtable events which allowed more interactive discussions around particular themes. The roundtables also provided opportunities for presentation of early stage ideas of projects.
Feedback following the event was incredibly positive, and we hope that some of the energy, enthusiasm, ideas and insights will continue to resonate through papers, collaborations and future events!
The event brought together people working with and affected by suicide to discuss and develop the approach.
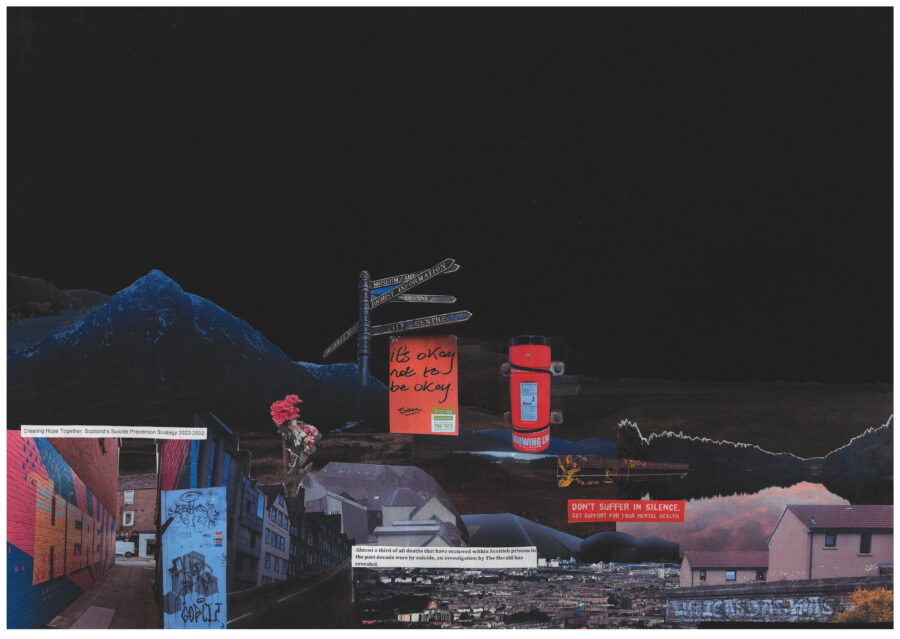
In line with our focus on the social and cultural contexts in which suicide is embedded, I presented some reflections on the relationship between forms of social-political and cultural ‘crisis’, including austerity, the cost of living crisis, transphobia, and suicidal crisis. I asked what the use of the term ‘crisis’ might conceal, particularly in relation to how many people’s experiences of distress and suicidality are bound up with longstanding, slow and more ‘unspectacular’ forms of violence, including being slowly ground down by unfeeling or uncompassionate structures, day by day.
Drawing on the idea of “creating a radically different cultural landscape”, as highlighted in the Time Space Compassion report, my presentation focused on some examples from ongoing ethnography with a community-based organisation, which I have pseudonymised as In the Open. In the Open provides support for people with enduring mental health challenges, through what I argued is a socially compassionate approach.
This included examples of:
forms of accompaniment offered by In the Open staff, though which they support people to access health and other forms of care
how In the Open operates as a space of inclusion and belonging for people who, for various reasons, are socially excluded and may even be positioned by other institutions and social structures as ‘burdensome’
how the long-term nature of the support that In the Open offers allows for the development of supportive, caring and trusting relationships between the members of the group, as well as with staff members
I also shared an example of the systematic denial of compassion to certain people, based on our analysis of the Fatal Accident and Sudden Deaths Inquiries (FAIs) of deaths by suicide that occur in Scottish prisons. My presentation reflected on how in these reports, many people who have died by suicide in prison are constructed as ‘difficult’, ‘non-compliant’ and ultimately ‘unhelpable’. I argued that many of these inquiries fail to engage with the broader uncompassionate environment of the prison and how this contributes to people’s distress and even death.
My presentation ended by asking people to think about and share examples of other socially compassionate or uncompassionate spaces and how these may be related to suicide or suicide prevention. This was taken up in smaller group discussions following my presentation.
Later in the day, I was in conversation with Haylis Smith, discussing the Time Space Compassion approach:
In May 2023 I was delighted to be featured as the speaker for the ‘First Thursday Seminar Series’ organised by the Centre for Creative-Relational Inquiry, in the School of Health in Social Science, at the University of Edinburgh.
This was a wonderful opportunity to share some thoughts, ideas and ongoing analyses from the pilot work that I did – along with Sarah Wright – for the Suicide Cultures project. We ran a series of arts-based workshops – testing out approaches to working with different community groups to have conversations about suicide, its meanings, and its effects. The audience was a broad mix of counselling and psychotherapy practitioners and researchers, as well other scholars of suicide, and the discussion afterwards was a welcome chance to hear how others connected with the findings, and our analysis of these.
The paper I gave for the seminar drew on some eclectic theoretical resources – Lauren Berlant’s ‘slow death’ and Avery Gordon’s ‘haunted’ sociological imagination – to think through some of the stories that were told about living with and experiencing suicidal distress in our workshops.
In this post I reflect on an instance of interrupting a discussion about suicide. I explore how asking different questions about the relationship between suicide and social inequality allows for different kinds of engagements with suicide. These kind of interruptions are simultaneously challenging, uncomfortable and necessary.
On the 17th of March, my colleague Sarah Huque and I attended an online roundtable discussion hosted by the Psychological Society of South Africa (PsySSA) entitled Suicide in South Africa: An Intersectional Dialogue. I was looking forward to the discussion, both as a researcher who works on suicide and as a research psychologist who previously trained and worked in South Africa.
I was particularly looking forward to the ‘intersectional’ focus of the discussion. The roundtable brought together the Operations Director of the South African Depression and Anxiety Group (SADAG); a mental health journalist who had lost her son to suicide; a psychiatrist; and a journalist who has survived “suicidal ideation/experimentation” (their words). The panel was attended by nearly 250 people, from across South Africa.
However, I was disappointed to discover that the discussion was dominated by a narrow, individualised, medicalised understanding of suicide. Someone repeated the phrase “the most dangerous kind of depression is an unmedicated one” and the psychiatrist proclaimed that “90% of those who die by suicide have a mental illness”[1]. The panelist from SADAG mentioned that since the beginning of the COVID pandemic they were experiencing a dramatic increase in calls to their crisis hotline but in the panel discussion there was no connection made between this increase and the particular social realities of South Africa, which has often been described as “the most unequal country in the world”. For me this was a clear and problematic missed opportunity to explore how the COVID-19 pandemic has intersected with existing social inequalities to make lives unliveable for millions of people in South Africa. This was but one example of the failure to engage with issues of inequality during the discussion.
By the end of the session I was feeling extremely frustrated and angry. In conversation with my colleagues in the Suicide Cultures project the next day, we reflected on how these kinds of discussions perpetuate decontextualised understandings of suicide. Spurred on by my colleagues’ shared concerns, I decided to write to the organisers of the event and express my disappointment. In my email I explained how I was especially disappointed by the lack of reflection on and engagement with the structural conditions which produce distress, in light of South Africa’s various intersecting legacies of inequality. I also noted that I felt PsySSA, as the representative body of psychologists in South Africa, had a responsibility to promote more holistic, ethical and contextually-relevant understandings of suicide rather than merely perpetuating individualised, psychiatric ones. I felt slightly better having, at least, articulated my frustration in this way but I did not have high hopes of a constructive response.
I was pleasantly surprised to receive a response a few days later acknowledging my concerns and inviting me to participate in a follow-up question and answer session. I was invited, during this session, to share my reflections on the initial discussion and to pose some questions to the panellists. I was both pleased and daunted at this opportunity to interrupt the discussion about suicide, especially as someone who is not a clinical professional. But I also felt a sense of responsibility to insert issues of inequality into the discussion of suicide, so I accepted the invitation.
I began my reflection by noting that the initial session had focused predominantly on identifying “signs” that people may be suicidal; promoting medication as the most effective treatment of suicidal distress; as well as suggesting that people who are experiencing suicidal distress can be protected using (coercive) forms of surveillance. I reflected on how these kinds of discussions are part of dominant ways of thinking about suicide, not only in South Africa but across the globe. I noted that it was important to expand understandings of suicide beyond these narrow focuses in order to more meaningfully contextualise people’s distress. Informed by many of the discussions we have had as the Suicide Cultures research team, as well as engagement with work of others in critical suicidology, I then posed the following questions:
How can we talk about ‘mental health’ and suicide in South Africa without centring issues of inequality and justice? By this I do not mean merely mentioning ‘social determinants of health’ or how some people’s distress may be caused by a lack of sense of safety in their communities, but rather what would it mean to reframe suicide as a social and political issue that is produced by social injustice, which demands social and political rather than merely individual responses?
What would it mean to shift from thinking about suicide as a mental health problem caused by depression to thinking about it as an expected and reasonable response to socioeconomic disadvantage or other kinds of social exclusion?
How do medicalised understandings of suicide and distress normalise social contexts which make life unliveable for many people?
How can we develop psychopolitical approaches which make connections between social inequality, injustice, and the emotional impact this has on people?
How can we shift from individual to collective efforts to repair ongoing social injustices?
Unfortunately, two of the previous panellists were unable to join the question and answer session due to load-shedding[2]. However, it seemed the questions I posed spoke to many of the challenges that South African psychologists and counsellors were facing, with many of them sharing their frustration about the difficulties of supporting people struggling with distress. There was also much discussion about inequalities in terms of being able to access mental health care, particularly for people living in rural areas. In this way, the critical interruption that I posed appeared to open up ways to talk differently about suicide. This was an important reminder of the power of interrupting normative conversations about suicide and how these interruptions can reframe suicide in relation to issues of social inequality. This is part of the work that we as the Suicide Cultures research team are doing through a variety of channels, including our seminar series, podcast and this blog.
[2]Load-shedding refers to scheduled rolling blackouts due to an insufficient supply of electricity, which is a relatively frequent occurrence in South Africa.
Do you want to learn more about LGBT+ youth suicide? Are you keen to think about practical strategies for prevention? Do you want to meet others who are interested in doing similar work? Come along to our event on the 24th November 4-6pm to find out more!