Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
[This project has now finished, but we will leave these posts here as a record of what we did]
The final stage of this project is now here – we’re working on our own piece of research! We’re looking at whether people’s episodes of depression are always visible in their medical records and if they aren’t, what are the reasons?
We’ve found out that when scientists do research into depression, their information on who experiences depression and how many episodes they have is often mainly based on their medical records. We want to find out whether people’s medical records are a good measure of that, or if a lot of information is missed by using them as a measure, because people may not always go to a doctor for their depression.
We’ll be doing that both on a large scale by analysing existing data, and in detail by asking people within the group about their own experiences of depression.
Within our group, we’ll be asking if people have always gone to the doctor when they’ve experienced depression, and if not, why not?
We’re also looking at data from the cohort studyUK Biobank, which has asked its participants to fill in a questionnaire to screen for depression and also includes their medical records, to see how well the results of the questionnaire match up with the medical records. If someone has a score on the questionnaire which suggests they are depressed, is there usually also a record that they have seen a doctor for depression at around the same time?
To help us refine our final question into a small piece of research, last week we held a Q&A with three researchers who study depression and work with cohort studies. Alongside quantitative research using cohort study data, we’ll also be able to do research looking at the lived experience of Depression Detectives members, and this week we were joined by social psychologist and research consultant Petra Boynton, to help us figure out how to do that.
Q&A
Hi Petra!
Petra: Hello and thank you for inviting me! I’m a Social Psychologist and Agony Aunt and my work involves teaching other people to do research, or how to use it in their own lives.
Tonight my job is to help you all think of ways you can take your research forward, particularly focusing on some of the practical issues to consider and how to make that work useful for you.
If you’ve got any questions for me please ask!
Depression Detectives member E (DD E): Hello Petra, how do you begin to design a piece of research?
Petra: Thanks, that’s a great question! It really does depend. Sometimes research questions are very clear and from that it’s quite straightforward to design something. Other times people struggle as they have loads of ideas so aren’t sure which to pick or have one big idea that’s very difficult to fit into a clear research question. Conversations, reading, reflecting and endless cups of tea seem to be the main ways into designing questions 🙂
Petra: My opening question for you all is to find out about what you’d like to get from this research. Sometimes it helps with the planning to have noted your motivations, hopes and dreams for a piece of work.
DD I: Great question. In an ideal world, what would happen as a result of us doing this research?
Petra: I’d love to see with any research, large or small scale, that it makes a difference that those who were involved in the research can observe or benefit from. What would others in the group like to happen?
DD M: Ideally I’d like to see an improvement of practice if possible
DD I: So people go to the doctor every time?
DD M: Or don’t. Is there a way for a healthcare professional to check in with you rather than assume all is OK because you didn’t go back?
DD I: Good point. So the onus is not always on the ‘patient’?
DD M: Yes, but I feel it should be a 2 way process as well. Not so difficult to get an appointment if you feel you need one either.
With the necessary change to in person consults over the past year, is there anything that worked well and could be continued?
I appreciate it won’t always work, but providing more options must be better?
I can’t think how any of this links to our question though – sorry
Petra: It doesn’t have to link to your question currently. If your question is to explore the difference between self-reported incidents of depression and what’s on the patient records is once you’ve compared these you could begin to explore solutions, and make recommendations like you have done above (if appropriate)
DD E: Well the point of research is to improve services. In terms of this current piece of work, being a complete novice, I have found myself enjoying learning late in life more and more about mental health research, and it feels a bit like a jigsaw puzzle that slowly but surely it all fits together. Designing our own research therefore is the last piece of the jigsaw and another learning curve. The end result for me would be moderate changes to the mental health system.
Petra: That’s a great way of putting it. Pieces of the jigsaw puzzle are always important and it’s a better goal than trying to make an entire jigsaw! 🙂
DD E: I could do with more clarity on self-reported and health records. May not be appropriate for this discussion on designing a research study – are we all singing from the same hymn sheet?
DD I: That is a good point about definitions
DD C: If we wanted to do a focus group (by writing rather than talking within our Facebook group), what would you suggest we do to make it real research and not just a discussion? What are the processes of such research? How would we best analyse what people have written?
Petra: Text based conversations are very valid and rich, so really the key to making them more robust is to have very clear guidelines on what the group will be discussing, how to treat one-another, explaining about confidentiality and also listing what questions will be asked. From that the data is in some ways easier to analyse as it’s already transcribed – but you would need to check through it to note what is and isn’t going to be included based on what kind of qualitative analysis you’ve selected.
Christine: Thanks. What kind of qualitative analysis would you recommend for text-based focus groups, or which ones would you choose from?
Petra: It depends. I think people sometimes get confused with text-based data that it can’t be analysed in any of the many ways you could use for qualitative research. Often they believe only content analysis would be appropriate because the data is derived from text-based chat. However if you think about how focus groups are usually recorded then transcribed, the text based chat is cutting out the transcription, it’s presenting you with a transcript or script.
In that case your choice of qualitative analysis would be based on your research question and theoretical stance.
DD E: I’m interested in the question of anonymised data! Is it standard practice in academic research and what methods are used to obtain anonymised data!
Petra: It really varies. Traditionally social science research has anonymised data either by ensuring those in qualitative research are given pseudonyms and identifying information is removed. Or in the case of quantitative research people’s responses are collated in numerical data. However, in some areas of research people don’t want to be anonymous, they want to be heard telling their story. So that can introduce some interesting dilemmas for them.
DD I: As a reminder, our winning question is:
“How does chronic depression/dysphoria differ from, say a single episode, or discrete episodes of reactive depression? Are there markers (biological, psychological, behavioural, and current or in a person’s history, e.g. trauma) that distinguish them?”
But this is too wide to be a research question.
What defines a good research question for a focus group or survey?
Petra: It’s a fascinating area to begin with but I agree it is very wide. And in its current form it may not necessarily lend itself to either a questionnaire or focus group, so the question may need adjusting to suit the method. A good question for a focus group or survey to answer is one that is specific but allows people to reflect and share.
So in this case you could look at psychological and behavioural aspects through a survey and map that to medical history. A focus group would be more likely to give you lots of rich descriptions of living with depression so would again be useful but if you wanted to link that to chronic depression it would need a specific angle.
DD N: We’ve done some narrowing down in the group and it’s likely that our final piece of data research will involve comparing medical records to self-reported data in cohort studies, to see how accurate medical records are as measure of people’s experience of depression
DD S: But we were interested in why self-reported number of episodes might differ from what people’s medical records say. If people aren’t going to the doctors with some of their episodes, why is that?
DD I: The data science answer will be pretty dry (eg x% of self reports are recorded in medical records).
How might the group add richness to this?
Petra: Which would be really important to note and, I suspect very common. A focus group would let you explore the ‘why’ aspect to this. So why is it people’s medical records and self-reported episodes differ?
A survey might let people note how many episodes they have had where they did and did not go to the doctor, and what they did to self-manage if they did not go, plus their reasons for not going (e.g. couldn’t make an appointment, didn’t feel previous care helped etc).
DD M: I feel like I don’t know enough of what’s out there, to know what we don’t know! If you see what I mean
DD I: We also talked about private (paid for) options in the group.
Petra: The positive thing about the existing dataset is re-analysing it will explore things it hasn’t already done. Also it already exists as something detailed to interrogate. It’s assumed the records do accurately describe experiences of depression. It might be your research confirms this – but equally it may show that recorded incidents of depression are well-below what people experience you can make suggestions for improving care accordingly.
DD C: From the group’s discussion, there were some more specific areas that have come up as possible topics for focus groups or surveys, related to the question on single episodes vs recurring depression. Would you say some are more easy to do or more suitable than others?
– We could discuss if those with an experience of depression in this group have gone to their GP for all episodes of depression. If not, what did you do/ where did you get help if it wasn’t through the NHS?
– What made you decide what kind of help to seek? Which factors did the decision where to seek help depend on?
– Which episodes of depression did you seek help from GPs from – the first, a later one, all, the most serious, the one that you couldn’t link to situational causes…?
– How do people’s experiences of the help they received from the NHS influence their decisions to seek help when they have a relapse?
– How useful are questionnaires to measure depression, and how could that affect detecting single episodes vs. repeated episodes of depression? We could have a focus group discussion on a particular questionnaire and formulate/ highlight potential shortcomings from a bottom-up perspective, which might lead to a future review of the questionnaire.
Petra: – We could discuss if those with an experience of depression in this group have gone to their GP for all episodes of depression. If not, what did you do/ where did you get help if it wasn’t through the NHS?
This might be a useful discussion to have as a focus group as it would indicate the reasoning behind not seeing a practitioner, which you could incorporate into a survey that in turn you compare with health records.
– What made you decide what kind of help to seek? Which factors did the decision where to seek help depend on?
That could either be covered in a focus group or survey but it potentially is more closed (or you could provide a series of closed responses) so that could suit a questionnaire well.
– Which episodes of depression did you seek help from GPs from – the first, a later one, all, the most serious, the one that you couldn’t link to situational causes…?
Asking about when they did seek help is good, and again you could quantify this so they could indicate which ones they did (or didn’t seek help for). The problem you may experience is putting a timeframe on this and relying on people’s memories. So if you want to ask about this and map it to health records it will need to be as precise as possible.
– How do people’s experiences of the help they received from the NHS influence their decisions to seek help when they have a relapse?
I’d say this would be better as a focus group, although there’s also a lot of evidence particularly from experts by experience and groups like Mad Covid and Recovery In The Bin who have documented this. So instead of asking again it might be better to draw on that evidence?
– How useful are questionnaires to measure depression, and how could that affect detecting single episodes vs. repeated episodes of depression? We could have a focus group discussion on a particular questionnaire and formulate/ highlight potential shortcomings from a bottom-up perspective, which might lead to a future review of the questionnaire.
I think that could be very interesting, and it would match existing research that has criticised depression screening tools. However it would be quite time consuming to do well, so as a general discussion it might work but to extend it into research it might be more complex
DD M: What constitutes an episode of depression? Will this be defined?
DD C: Definitely something worth exploring! In the data science q&a we were told that it’s up to 2 years, but there was no answer as to who decided this and why it was defined that way.
Petra: That’s an excellent point, you would need to define this. And it may be you use an existing measure of depression to get this information.
DD M: Yes there were 3 categories I think? So which type of depression would we want to focus on? I think this might help us narrow down the question
Petra: Something to think about is if you do the research if it could be criticised. People often panic about this idea as they fear it means their hard work being disrespected. What it means is whether other people might have questions or concerns about the research or notice barriers or limitations. In this case however you want to measure depression it would need to be something all participants understand and would respond to similarly. For example ‘major depression’ might be interpreted in many ways so you will need to define it for all.
Petra: If your plan is to Answer the question “Compare self-reported data to health records”. How might people think that would work in practice?
And as a follow up to this it might help to consider what you think the research might discover. My guess would be that self-reported data would suggest a far higher incidence of depression than what is on health records. But what other possible outcomes might there be? If you can consider these it will help you shape your question and how you’d like to answer it.
DD M: Petra, good evening and thanks for being here. What tools do you recommend for the analysis of qualitative data? Thanks
Petra: It really depends. Some people like to use qualitative data analysis software like Nvivo or Qualtrics, whereas other people do the analysis manually. If you don’t have a large dataset the latter may be a better option. I’d suggest if you plan on doing qualitative research then another session like this with a qualitative researcher might be good to help you think about ways to analyse and interpret your data.
DD N: We’ve got about nine minutes left folks!
Petra: I’m not sure if we’ve covered everything people would like to ask. But my advice would be if you want to compare self-reported episodes to health records you need to find a way to match self reported depression with what’s on a health record. But in a way that is robust and transparent.
For example people will know they are self-reporting, but if they already know what’s on their record they may over or under-estimate their self-reporting so how you present that information may need to be carefully managed.
You’ll need a clear measure of self-reported depression over a set period of time (to match the existing health record).
That sounds simple – to match self-report to the health records, but it’s surprisingly in-depth.
Once you know the direction the self-reporting corresponds with the health records you could run a focus group to explore the findings, what they mean, why you think they have happened in the way the research indicates, and what recommendations might be made for improving care.
DD N: That’s all we’ve got time for I’m afraid! Thanks so much for coming Petra, this has been really interesting – a lot to think about!
Petra: Thank you for having me! I always find these conversations leave us with even more questions so if after this evening you are still unsure or have other things you’d like me to answer please let me know and I can get you more information. I think this is such an important piece of work and I’m really looking forward to learning what you find out!
To help us refine our final question into a small piece of research, yesterday we held a Q&A with three researchers from the University of Edinburgh who study depression and work with cohort studies: Mark Adams, Alex Kwong and Matthew Iveson
Q&A
Hi all!
Mark: Hi, everyone, I’m a statistical geneticist (meaning I use maths and computers to study genetics). I work on very large scale genetic studies of depression, comparing DNA between people with and without depression using data from countries all across the world. I’m also interested in how depression symptoms might or might not relate to each other.
Depression Detectives member I (DD I): Which cohorts do you work with /have access to for this project?
DD S: What are the timescales of each of those? (Sorry I know you’ve posted links but I haven’t had as much time to read for this as I’d hoped). The longer the better if we’re looking at recurrence of depressive episodes over lifetime…
Alex: Do you mean the timescales for completing the research or how long the data has been collected for?
DD S: How long the data has been collected for
Mark: In Generation Scotland, our initial measurement was retrospective (asking people to recall past experiences) and they can be initially grouped based on that response. 10 years later we asked the participants again, so it would be possible to look at people who initially did not report an experience of depression, but did have an episode subsequently. UK Biobank is similar, with a 5 year gap to the follow-up. The other way to look at it would be using health records (hospital, GP, and prescribing).
Alex: So in UK biobank we have data collected at multiple waves across ~10/12 years. In that time people would have been asked to think back about how many episodes of depression they had (which can be problematic as you might imagine). In Generation Scotland there is a similar method where people have been followed up over time but have been asked this specifically. There is also the possibility of linking to health records as well which could provide further validation for these self reported measures.
Matthew: Hi all, I’m mid bedtime with my 3 year-old so apologies if I have to duck out. I’m a researcher in the Psychiatry department focussing on using routinely collected health data to examine life-course risk factors and mechanisms underlying depression.
DD S: Sorry! We found with my last project (with parents of small children) that we needed to put the Q&As quite late, or everyone was still doing bedtime. Baby books lie!
9pm is quite impressive for a three year old though.
DD C: I was just feeling proud of myself for extracting myself from my 7 year old’s bedroom in time to be here!
DD M: We managed 8.40pm with ours. Whoop!
DD S: My 7yo is still up, but he’s watching TV…
Alex: Hi everyone, I’m Alex and I’m a mental health researcher like Mark and Matthew. I normally work on data from young people and look to see how depression changes across adolescence and why there are different patterns of depression for some people and not others. I normally look at genetic and environmental factors like childhood trauma, bullying and relationships. But then more complex factors like parental depression which could be a mix of both genetics and the environment.
DD C: How do you even begin to untangle all of that?!
Alex: With great difficulty that’s for sure! We don’t tend to do all of it in the same piece of work. Normally we will have a specific question like how does parental depression impact on their children and try to examine that specifically.
DD C: Sounds like the only possible way! What research methods do you use to investigate these questions?
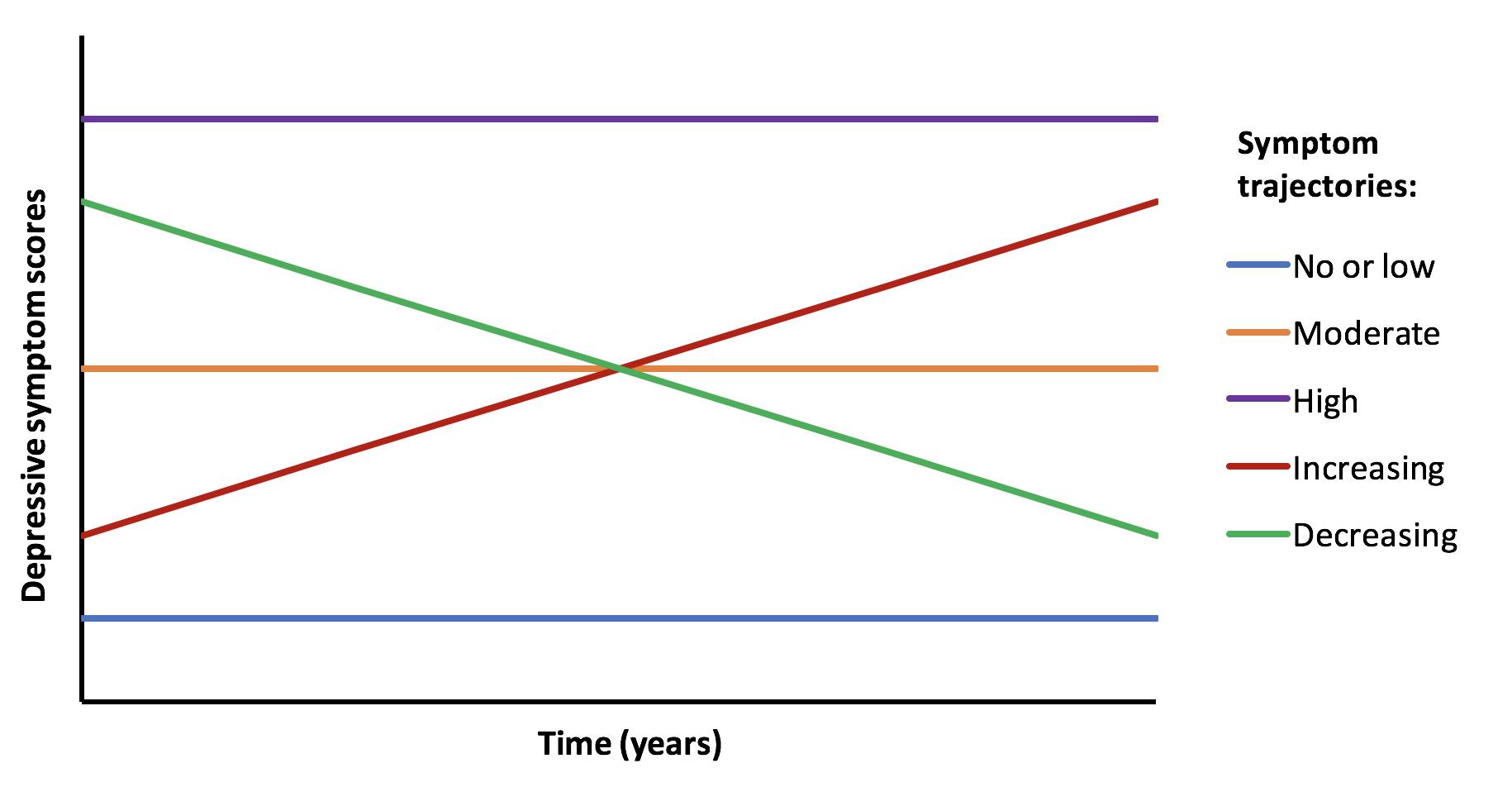
Alex: Excellent question. So there are multiple methods but my preferred method is to look at trajectories of people over time.
So let’s say someone completes several questionnaires about depression over time (maybe every year for 4 or 5 years), we then create a trajectory for that person. If you have 100 people then you have 100 trajectories and you can start to see how people differ and if these are specific characteristics for different groups of people.
So you may have something that looks like this image below.
DD C: I’d be really interested to see how you ask about depression. I know that my personal experience of depression is very different to the questionnaires I was supposed to use for screening when I worked as a medical doctor.
Alex: So each cohort is different and that is one challenge. But I have used this measure quite often – the short mood and feelings questionnaire. It was mainly aimed at looking at depression in children and adolescents, but can be assessed for older people as well. It’s definitely not perfect but on average those who score higher on this questionnaire are more likely to meet the criteria for depression assessed by a GP
DD C: Thank you for sharing that. It looks pretty standard. I really find it hard to reconcile these questions with my 40 years of experience of being depressed and would be interested to hear if others agree. For me, it went far deeper than that and this sort of questionnaire only scratched the surface. I am also prejudiced against it as I found many patients in elderly care medicine were labelled as being depressed on the basis of a questionnaire like this, whereas the truth was that it was perfectly rational and reasonable for them to feel low and hopeless when they were trapped in a hospital bed for months on end and the appropriate treatment was not to give them SSRIs!
Alex: Yes I can see your point. I think the questionnaires just scratch the surface as you say and there is a lot more detail that could be asked.
DD C: I guess the added detail would negate their use as a quick screening test though. On the other hand, I think there is a difference between the sort of depression which is encompassed by those questions and the sort which is more complex and this is relevant to treatment, given that some depression may be adequately treated by standard GP options, while other forms require years of talking therapy plus whatever else.
Alex: Yes it’s a double edged sword really and as you say there is like an academic version of depression (assessed through these quick fire questionnaires) and then the actual real life depression that people face on a day to day basis.
DD C: My biggest concern with this research question is how to recruit the single episode group. From the survey you did, we’re a bunch of long-haulers! How would we attract people who have had a single episode in the past and interest them in becoming part of our study? And how do we know that it’s only 1 episode and they won’t relapse again in the future?
DD E: Perhaps we need some kind of “survival analysis” for time to next episode?
Matthew: It’s totally possible to run -time-to-event’ studies with multiple events. It gets tricky depending on the variation in number of events, so an alternative is to break down ‘classes’ of trajectories – are those with 1 episode different to those with 2-3 episodes, and different to those with 4-8 episodes, etc.
DD C: That’s an interesting thought. I guess the only way we can know it’s a single episode is to follow them up until death, which isn’t exactly practical! Maybe what we need to look at is the difference between people who dip down occasionally and infrequently but are well between episodes versus those who are chronic?
DD E: Or have another endpoint, like 15 years worth of follow up. This is how things like cancer recurrence are studied. But i appreciate Matthew’s point about the scale/trajectory/frequency of depression mattering too.
DD E: There must a wealth of data in Medical Records at the Royal Ed of one-off receive episodes as well as CDD
Matthew: I think some of the GP and hospital records for Generation Scotland go back to the 1980s, though I can’t guarantee their quality or useability
DD C: Yes, I can see that a lot has changed in psychiatry since the ’80s, so that could be a very messy process to embark upon….
DD I: How do you define single episode? What does it look like in your data?
Mark: Defining a “single episode” is difficult. When does an episode “end”?
DD E: Do the data you study have groups of folks who have single episodes of depression and another with multiple episodes? My hunch would be most patients are in the latter category, but maybe the data can’t say so, or say otherwise.
Mark: We find in our data about an even split between people who only report a single episode and those that report more. It would be interesting to compare health records between the two groups.
DD N: Surprising (to me anyway)! Is that based on self-reporting or GP records?
DD S: I’m sorry, I didn’t see the papers you’d shared below until a few minutes ago. I’m just having a look now. Is chronic depression just being depressed forever (rather than it coming and going)?
Matthew: Chronic is generally having diagnosis-level symptoms for 2 years or more, affecting you for more days in a week than not.
DD I: Part of the question is about single episode vs chronic depression /multiple episodes.
What measures would capture that?
Matthew: It’s always worth thinking about “in an ideal world, how would we measure that”. The best way would be to follow people over time and ask them about symptoms of depression that they’ve recently (rather than having to recall an experience that may have happened years or decades ago). Unfortunately there are no large genetic studies with such short follow up intervals. ALSPAC probably comes the closest, followed by whatever information we can glean from health records in other cohorts.
DD I: Within ALSPAC did they ask both parents?
When the kids got old enough, did they get the depression questionnaires too?
DD I: We have had some discussions in the group about what is not captured by GP records (for various reasons).
You mentioned in the group that ALSPAC asks people to fill in depression questionnaires regularly.
Could these be compared to what is in GP records? Eg suspected depression from questionnaire data vs confirmed by gp
DD C: Are we able to get hold of their depression questionnaire to see what they ask? That could be a good starting point…
DD I: Is the questionnaire online?
DD M: There’s a standard depression questionnaire… GPs also use the depression forms. I think PHQ9 is the one I know
DD C: I’d be interested to know what other people in the group make of the standard GP questions as I found they were a very blunt tool and didn’t encompass my lived experience of depression at all. Maybe I just had a different form of depression to the standard version!
Alex: You could compare self reported depression from a questionnaire to GP records. But there are some things to bear in mind. Firstly, not everyone who has an episode of depression will go to their GP. So you may be missing information there. The opposite could also be true in that someone may go to their GP when they’re depressed, but may not fill in a questionnaire because the survey wasn’t asked at that time.
DD C: Are GPs supposed to carry out the standard questionnaire and put the result in the records or do they just use their clinical judgement? If the latter, then is the diagnostic process powerful enough for it to be included in serious systematic research? It’s been a long time since I bothered going to the GP with a depressive episode, but when I did I was never formally assessed. The first time, the GP took great pains to differentiate between whether I would walk out of the way of an oncoming bus or whether I would step into the path of said bus etc etc, but I have never been asked the standard questions such as I learnt at medical school. My understanding of clinical research (I also used to be a researcher, but that was cellular and molecular so very different) is that you need to standardise the diagnostic process.
DD M: In my experience it varies
Alex: So I think GPs can put scores from a questionnaire on health records. This is actually quite common for those with perinatal depression. That said, my understanding from talking to a lot of GPs is that it’s a bit time consuming to run these questionnaires and it’s better done by primary or secondary specialist care.
DD M: Interesting 🤔 I think PHQ9 is really quick, but maybe not for the first time
DD C: Fair point, but does that mean that GP records are less valuable as a means of research data if the diagnostic process is, how shall I put it, non-standardised!
DD M: Could we not look at prescription data in that case?
It would be skewed slightly by use for other conditions though. And we’d have to be v cautious re amitriptyline as its also used for certain types of pain relief
DD C: Only if we are only investigating depression which has been treated by medication. I stopped taking anti-depressants a long time ago but had several episodes which I managed without drugs and without seeking help from my totally useless GPs.
Matthew: Prescribing data also covers therapies and social prescribing (as long as they were prescribed)
DD C: But only if prescribed by the GP. This assumes that everyone’s treatment is being coordinated by the GP or another NHS professional. We don’t know how many people give up on their GP after years of ineffective treatment and go off and sort themselves out, like I did. I would never want my GP records to be used in serious research because they would give such an incomplete picture.
DD S: One basic question is, as far as the research literature goes, what proportion of people do you think have one single episode, vs have several episodes?
And is there a typical pattern to that? (Like, age of first episode, frequency of episodes, etc)
Matthew: There’s a bit of a problem in terms of how you define an episode, generally. A person with chronic depression could look like they are having one long episode (2years+), and are very different to the typical ‘episode’ of depression in major depressive disorder. If you look at health records (e.g., prescriptions) you can estimate episode numbers and lengths, but it’s only ever an approximation
DD C: In what way do you think we could best define or operationalise the term “episode”?
Matthew: I think taking it literally is best. An episode can be any length (though the DSM criteria is min of 2 weeks), but when that length gets above 2years then we should be calling it chronic
DD S: When you say chronic depression, does this include dysthymia, or is it a chronic version of more severe depression? And do you think these differ qualitatively, or only by degree?
DD M: What’s the difference between major depressive disorder and chronic please?
Matthew: I’ll preface this by saying I’m not a medical professional. My understanding is that major depressive episodes are sufficient depressive symptoms lasting 2weeks+, major depressive disorder is having 2 or more episodes, and chronic depressive disorder is having symptoms for over 2 years. Dysthymic disorder is a little confusing, as it is often lumped in with chronic, but many consider the symptoms to be lesser in dysthymic disorder
Mark: Major depressive disorder includes somatic and cognitive changes as well (extreme changes in sleep, diet or weight, or lack of energy and concentration) whereas chronic depression could occur with only the symptoms of low mood and lack of interest in activities.
DD M: Aha, that’s really interesting. Thanks
DD S: That’s interesting, ‘chronic’ by that definition does sound more like dysthymia. It also raises the question of whether there are qualitative differences in the pathophysiology, between people with the somatic and cognitive changes too, and people with only mood issues – any thoughts on that?
Mark: Yes, the non-mood symptoms all implicate circadian rhythms.
I think somatic and cognitive changes are a bit different because they are more liable to snowball (poor sleep leads to fatigue, which causes concentration problems, etc)
Sarah: Hard to tease out cause and effect as you could argue ways that all 3 types of symptoms affect the others…apparently the cognitive ones often don’t fully remit between episodes, despite mood improvement (to allowing normal fluctuations within ‘healthy/normal’ range) so are they independent to at least some degree?
DD E: I hope this is an appropriate question – Where does Bipolar Depression rank in Long term depression?”
DD L: Bipolar is often considered separately in research studies, so it would depend on the study but often a study on long term depression wouldn’t look at bipolar.
DD N: Something that’s come up in talking about this question is how you measure how many episodes of depression someone has had, since not everyone will go to the doctor every time they have an episode – do you know if there’s any existing data on how those things compare?
DD M: Plus I think relying on self reporting will be unreliable
Alex: Yep self-reporting isn’t very reliable, but it could give more depth than the questionnaires – it can pick up on things the questionnaire designer hasn’t thought of. Plus even knowing that there is a difference between what’s recorded and how people perceive their medical history is in itself interesting (just doesn’t tell you the cause of the discrepancy)
DD S: This is what I am wondering. If ALSPAC is giving people a depression questionnaire once a year, that could pick up episodes of depression that people don’t go to the doctor with (and therefore would be invisible to electronic health records). Has anyone done that analysis? Comparing depression according-to-the-questionnaire to depression-according-to-health-records for the same population, and seeing how they differ?
Alex: Nobody has looked at this yet but this would be an interesting option and something that could be done.
DD S: I wonder what depression questionnaire they use – does it cover the last year, or only how participants are feeling at that moment?
Alex: In ALSPAC, depression is measured using the short mood and feelings questionnaire when assessing depression in young people and then the Edinburgh Postnatal Depression Scale in the young people’s parents. Even though it says postnatal, it can still be used when people are not pregnant. These are self reported questionnaires and can be completed quickly. There is diagnosis data from more advanced screening measures as well but these are the most commonly assessed in this cohort.
In Generation Scotland, a different measure called the GHQ28 is used whilst in UK Biobank, the PHQ4 and PHQ9 are used.
DD S: So just at that time then – could miss any depressive symptoms that occur between the yearly questionnaires?
DD N: Do you think it might be possible to extrapolate from that to an idea of the total number, including people who had a depression episode at other times of the year?
Alex: In regards to timing, most questionnaires will only capture the last 2 weeks or the last month. So this poses some problems like what if you catch someone on a bad day? This is an example of measurement error which is a really common problem we have in mental health research
DD M: Catching someone on a bad day would be better than on a good day though?
Alex: I think it extends both ways and both ways are potentially a problem depending on your point of view. Good news for the person if they’re having a long episode of depression and have a good day (hopefully the start of more good days) but bad from a researcher point of view if it’s just a good day in isolation and an anomaly with regards to the data.
But essentially yes, this is a problem sometimes.
DD L: Is there any existing research on predictors of chronic depression or dysthymia? Just found this article – are we thinking of doing something along these lines?
Matthew: There’s also a recent paper from a Brazilian cohort (all middle-aged civil servants, only 2 waves) that shows education and female sex predict persistance
DD S: Well we definitely aren’t going to be able to follow people for 11 years! We’ve got, like, two weeks… But we do have access to the data several cohort studies have been collecting, so we can ask questions of their database…
DD I: With our question as the starting point, what question would you ask the data?
Mark: I’d start by seeing if we can use health data to differentiate people who reported (retrospectively) having single versus recurrent depression to see how closely that data matches what people remember.
Health data is what we call “prospective” because data collection started before the event you want to capture occurs. This will not be totally true because health records only go back in time so far, but there are some statistical methods we might be able to apply to get around that.
Alex: I would agree with Mark. If there is the possibility of using self reported data AND health records, then you can verify if the two are correlated and be more confident in your data.
DD S: I thought we have the (anonymised) records from the cohort studies, but there’d be no way to identify and ask those specific individuals about their perception?
Matthew: I think once we’re happy to use health records to estimate episodes and that it’s reasonably accurate, then a simple question would be something like “what does a life of episodes look like? How are they spread out, when (in life/year) do they occur more frequently?” and also “What risk factors predict more episodes?”
DD S: My concern with looking at the pattern alone, is whether it would add anything novel, although I’d be very interested in the result! But if we look at patterns in combination with risk factors, or treatments, that might be useful? I’m just not sure what’s been done already. That said, being in the UK might be novel (healthcare system different from other countries), also the combination with risk factors / protective factors / treatments that worked or didn’t, might add useful information?
Matthew: I think Mark Adams is talking about comparing the questionnaire responses that the cohorts have already completed (including several waves of depression questionnaires) to the health records we have for them. If someone reports a depressive episode in the last 12 months can we see this in their health records?
DD I: Our question speaks to biological, psychological, behavioural and history eg. trauma.
This is pretty wide.
What do you think might be the key to the difference between single episode and multiple/chronic. (Even just a hunch)
What measures do you have within the cohort studies that might speak to that?
Mark: Based on what we know from family data, my hunch is that single episodes of depression are more situational.
DD L: Yes, I would expect people with higher early life stress to have more chronic depression, with single episodes linked to a stressful experience in adulthood but less early life stress.
DD E: I would like to ask what method of study will the survey take, qualitative or quantitative?
DD L: It depends on what the specific research question is. Pretty much everything the panel talked about tonight would be quantitative because it would be using large amounts of numerical data.
DD S: From the Generation Scotland paper you linked to, “We found that the heritability of recurrent Major Depressive Disorder illness course was significantly greater than the heritability of single MDD illness course.” Do you think that means that a single episode of depression is almost a thing that could happen to anyone if the right (wrong!) circumstances come together. Whereas recurrent depression is more to do with people having a genetic vulnerability to it?
Mark: Yes, that’s a good conclusion. Also about 75% of the genetic risk is shared between single and recurrent, meaning that the genetic vulnerability is very similar.
Alex: I remember reading a paper which I think said that multiple episodes of depression had a stronger genetic basis compared to those who had only one episode. I think it was a paper by Kenneth Kendler using some data on twins.
DD S: When discussing our question, one big reason for people wanting to know the answer is the hope that if there were ways to predict at first episode which people would have a one-off and which would be likely to have repeated episodes, then maybe those groups could be treated differently.
Do you know if GPs or psychiatrists ask people if they have family members who’ve experienced depression, when they are diagnosing them?
Matthew: There is certainly a READ code (one of the codes GPs use when entering a record) that is for family history of depression, but whether it’s used (due to time limits) or accurate, who knows. It would be possible to check accuracy by comparing to cohort questionnaire data, as Mark Adams suggested above
DD C: I’m beginning to wonder whether our research could be to do interviews with people who have a history (current or past) of depression and see whether their experiences are adequately assessed by the standard questionnaires!!! I’m not being completely flippant here, since I think the relative triviality of the questions reflects the lack of adequate treatment options….
Matthew: The problem with that approach is that clinicians and researchers really do need standardised questionnaires. They may not be the best, and they may not suit all cases, but they allow us to compare between studies/populations/countries.
DD N: I guess perhaps the question is then whether the standard questionnaires could be improved! I’d be interested to know how long ago the current ones were created
DD C: I know. I guess I’m just a bit cynical because I don’t feel it applies to me and because I have witnessed so much inappropriate use of them….
DD S: Also, in practical terms, that would probably need a new ethics application and we probably can’t do that in time.
DD C: Do you think it would be interesting to have feedback from our group on these questionnaires?
Matthew: I think that would be great: most of the questionnaires were designed by clinicians. I would say constructing a more patient-led questionnaire is fantastic, but would take a while – probably more time than you have here. Something to come back to, though!
DD C: I’d certainly be up for it if you ever wanted to attempt it!
DD C: Maybe we could pick out some questions , even if it’s not the full questionnaire…
DD N: I’m afraid that’s our hour and we’ll have to let the researchers go now – thanks so much for coming Alex, Mark and Matthew
Alex: Thanks for having us! Really interesting to talk to you and discuss these ideas!
DD S: No. Lock the doors. Stop them from leaving.
(OK, I’m joking.)
Thank you for coming Mark, Matthew and Alex, it’s been fantastic and so useful.
DD C: Thank you all so much! It’s been really enlightening
Matthew: Thanks everyone, it’s been great. It’s tough to nail down a research question – happy to come back to this and any other questions another time.
Over the last couple of weeks, the members of Depression Detectives discussed the top 10 questions we chose from our list of 59 possible research questions, then voted to choose the one question we’ll be using to design a small piece of research which will be done by the group.
The winning question is…
How does chronic depression/dysphoria differ from, say a single episode, or discrete episodes of reactive depression? Are there markers (biological, psychological, behavioural, and current or in a person’s history e.g. trauma) that distinguish them?
The next step is to narrow down this quite broad question to something it’s possible to try and answer in a small piece of research happening over a short time. That’s what we’ll be doing over the next two weeks.
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with three researchers from the University of Edinburgh who study trauma – Karen Goodall, Hope Christie and Rachel Happer.
Q&A
Hi all!
Karen: Hi everyone! I am Karen Goodall. I am a senior Lecturer at the University of Edinburgh. My research is focused on childhood adversity attachment and wellbeing and mental health in adulthood.
It’s really great to be here – we are looking forward to chatting with you!
Hope: Hi everyone! Thanks for coming along this evening 🙂 my name is Dr Hope Christie, I am a Global Challenges Research Fellow at the University of Edinburgh, which is a long winded way of saying I do a lot of work with people in different countries – mainly South Africa.
My work focuses on parents who have experienced something traumatic and may have developed post traumatic stress disorder (PTSD) as a result. I’m interested in how parents feel their trauma and PTSD has affected them, their parenting and their family dynamic.
I’m also excited to be here chatting with everyone this evening!
Rachel: Hi everyone. I’m Dr Rachel Happer. I’m a Clinical Psychologist. I’ve spent the last twenty years working with children, young people and adults who have experienced trauma, particularly trauma that has occurred within interpersonal relationships. My research interests are compassion, shame and institutional roles in abuse.
Depression Detectives member S (DD S): Hello, thank you so much for coming!
For starters, what are the ‘headlines’ of the relationship between trauma and depression?
Rachel: Depression is often the outward symptoms that someone might see, trauma is the body’s response to experiences that are difficult to manage.
Karen: There are a large number of studies that point to a relationship between trauma and depression. Particularly trauma in childhood seems to be relevant.
It’s also worth mentioning that depression is one outcome but there are other outcomes linked to trauma such as anxiety disorder or substance use. But it is important to say that not everyone who has experienced trauma will become depressed and vice versa.
DD C: would you say this is mainly connected with attachment or other factors?
Karen: That’s a really interesting question. We tend to think of attachment relationships as risk or protective factors. Trauma seems to be more potent if it is interpersonal, especially if it is related to a parent. On the other hand a secure relationship with another person can protect against the stress of trauma.
I think I should also mention that insecure attachment relationships might play a role in developing depression. However, in children and young people there is evidence that the extreme stress of trauma can lead to impacts on the neurodevelopmental system.
It is also important to mention that we tend to think of trauma as ‘an event’. In fact trauma can be the absence of something, such as good parental care.
DD A: In the context of childhood traumas from parental care (or lack thereof), and given that these have a huge impact on mental health, what approaches could be taken to intervene at this stage? As children may not be able to identify that something wrong/bad is going on!
Hope: Just to add onto the great answers Karen and Rachel have given, it is most often the case that mental health difficulties such as depression and anxiety are often co-morbid or share similar symptoms to post trauma symptoms as well. This can sometimes lead to trauma symptoms being overlooked if you are going to your GP for example.
DD S: Does everyone who’s experienced trauma experience depression at some point? If not, why do some and not others?
Rachel: Each person’s journey through trauma is unique. Whether or how some experiences the impact of trauma will depend on many things including the supports they have around them, the response someone receives to disclosure of trauma, how quickly someone receives the right help, the other resources in their life, the scale and impact of trauma.
DD N: Does depression that stems from trauma present differently in any ways to other causes of depression?
Rachel: I would always see someone’s experiences as unique to them. Depression has some key features that have quite a biological underpinning and PTSD type trauma also has some key features such as flashbacks and nightmares.
However, trauma, particularly unresolved, can have a lifelong impact. Both trauma and depression can be impacted upon by the quality of a person’s relationships.
Hope: Great question! I would say that no, that there is no difference in the way that depression presents. Typically what we see is that depression comes second to the trauma. Depression and trauma do share similar symptoms to each other in terms of low mood, withdrawing from relationships or social situations, etc. But there are differences as well, in terms of the root causes of each and how we may treat them
DD N: Thanks for both of those responses. That makes sense. Does that then have implications for treatment of depression? For example making it more complex to get to the underlying issues. And what are the strategies that could be used to help get a diagnosis that reflects causes of depression as well as the depression itself?
Karen: This is quite a complex question. Generally, depression may have multiple causes but typically it will be the symptoms that are treated. I’m not sure that it would be too easy to get an alternative diagnosis but certainly having the space to be able to talk to someone about what happened to you would be the first step in starting to address core issues. Antidepressants can play a role and can support someone who is undertaking other types of therapies but you would also want to be thinking ideally about a therapy that addresses the core issues.
DD A: Can you give us a summary of what current literature tells us about childhood attachment and trauma related mental health issues in adulthood?
Karen: Great question! There is a very big literature on insecure attachment and mental health which shows that people who are insecurely attached are more prone to mental health conditions in general. This is because through attachment relationships we learn lots of skills such as how to regulate emotions, what we think of ourselves and the world and how we can trust other people. In this way, people who have a secure attachment may be a bit more resistant to stress, but if we haven’t had those experiences, we can be more prone to finding things stressful. This is one of the ways in which people can become depressed – through stress.
DD I: As part of our Top 10 questions in the group (as we try to narrow in on our 1 research question) we have:
How does chronic depression/dysphoria differ from, say a single episode, or discrete episodes of reactive depression? Are there markers (biological, psychological, behavioural, and current or in a person’s history e.g. trauma) that distinguish them?
Can you say anything that might speak to that question eg. research that has been published or gaps that still exist?
Rachel: Big question! Trauma is really about what has happened to someone, either in recent years and in childhood. Chronic depression, reactive depression and single episode all could have a trajectory that arises from trauma, particularly if trauma is not resolved. People often take many years to reach the most effective trauma focused psychological work.
DD I: We know. We are just exploring/trying to narrow things down in the group just now.
Do you know of any markers of trauma (other than the person remembering themselves).
What if it happened very young?
Karen: That is a very good question indeed because we tend to think that what we don’t remember can hurt us. However it is clear from the research that trauma in early life has a very pervasive effect. In terms of markers, I don’t think you could point to any specific presenting factor and say that it is related to trauma with certainty. What you might expect though is the usual symptoms of difficulties relating to others, making sense of oneself, being prone to anxiety and difficulties in regulating emotions.
DD E: Would these symptoms necessarily be flagged as trauma-related if the individual didn’t feel able to disclose? And separately, since things like struggling to make sense of your identity are often attributed to adolescence or just a part of growing up – at what point is that distinguishable?
Karen: On the whole, I think the impact of trauma tends to be under-rated. For example, when a person goes to a GP with depression, there is not usually the time to ask about what happened to that person in the past or currently and the symptoms of depression are just treated. It is very difficult for people to disclose a history of trauma and often they might not even see it as relevant to their current symptoms. But no, in general practice I don’t think they would be immediately recognised as trauma related. There is a big push currently to ask more about histories but it is tricky.
DD C: I’d add to this that someone may not define their experiences as trauma. It took me many years of therapy before I accepted that I had a traumatic childhood (disorganised attachment, no safe person or safe places….) and it’s only since accepting this term that I’ve been able to reframe things enough to recover. I guess what I’m saying is that it’s easier to define depression, since that’s a bunch of well-defined symptoms, than trauma, which relies on an account of what happened in the past. I wonder how this affects the ability to research trauma-related depression – who defines the existence of trauma in the history?
DD E: I have been in the same boat – I’d be really curious to hear the response to this one!
Karen: I couldn’t agree more. It is much easier to diagnose depression than recognise trauma. In terms of research, many questionnaires will not ask directly ‘did you experience trauma’ but instead might ask about more subtle things such as ‘did you fear either of your parents’. This type of trauma tends to be additive. From my own perspective, I am very interested in emotional abuse because some of the behaviours are ‘normal’ behaviours that happen in all families, such as swearing, shouting etc. It only becomes emotional abuse when it is at the higher end or carries on for a long time.
I also whole-heartedly agree that many people may not define their own childhood as traumatic as we tend to think it is normal. Recognising that you weren’t supported or you were exposed to potentially dangerous situations etc. can be a first step in understanding responses such as chronic loneliness, unmanageable fear or depression.
DD C: “some of the behaviours are ‘normal’ behaviours that happen in all families” and also we only have experience of our own families so we have no clue what it is like to be a child of parents who are less abusive. Another reason we can’t recognise our own trauma. So how does the brain know that it is being traumatised when the person is reacting to what is essentially a normal situation for them? I didn’t know that other families didn’t treat their children like that until I became part of my husband’s family in my 30s!
Oops, we were typing at the same time and you have answered me! 🙂
DD C: How would you address this issue of recognised/undiagnosed trauma? If people present to their GP and all they are offered is anti-depressants or 6 sessions of counselling, then no one will get to the root of the problem and yet another person is failed by the system….
DD E: Hello Can you explain what the impact is on the brain when trauma is experienced and does it contribute to dementia in later life?
Karen: I am not an expert on dementia. However, it is clear that when extreme stress is experienced through trauma, it increases what is called allostatic load – wear and tear on the brain and stress regulation systems. Trauma and multiple adverse experiences in childhood such as loss have been linked to physical health such as heart disease and diabetes. It would not surprise me if it were related to dementia but I have to admit that I don’t know this literature in much detail 🙂
DD I: Possibly slightly off topic (if so just ignore)
In our Top 10 we also have a couple of questions about parenting, if you are able to speak to those at all?
I think we can all agree that being a parent is a really difficult job and most of the time parents are really doing the best they can with the tools they have.
a) There is an extensive amount of literature covering depression and parenting. Pointing to parents (mostly mothers – as they have been most studied in regards to this topic) experiencing a number of impairments in their parenting particularly around the parent-child relationship/bonding, as well as being more withdrawn or irritable with the child. In terms of counteracting these effects, there isn’t a one-size-fits-all solution, but social support/support from friends and family is consistently found to be a good protective factor.
b) Again, parents work with what they have. If they themselves were never modelled healthy behaviours, positive coping strategies and emotion regulation in their own childhood, then it is unfair to expect them to be able to model that perfectly for their child. I would also like to add that perhaps depression/trauma/anxiety may impair certain parenting behaviours, but this does not mean that people are bad parents. They will still be trying their hardest and will want the best for their child. Therapy can help parents reflect on their own behaviours for them to model this for their child, but their child may also pick up these things from other family and friends around them as well.
Hope this answers your questions! 😊
DD E: This is somewhat of a broader question (and less in the specific scope of depression), but as complex trauma and C-PTSD was mentioned in the Depression Detectives group earlier – I’m wondering what your stances are on that topic? Specifically that effects of complex trauma can present in less “classical” ways (i.e. emotional dysregulation as opposed to flashbacks) and symptoms such as this emotional dysregulation and associated SI/DSH behaviour can end up being labelled as borderline personality disorder. Do you think that they are separate conditions, or just different names for the same thing? If too big a question feel free to ignore this!
DD C: I’m really interested in this, too, thanks for asking. I find it difficult to tell the difference between borderline and complex PTSD… I think, to me, it seems that borderline seems to mostly have underlying complex PTSD? Would love to hear the experts’ views on this…
DD E: This is especially interesting too due to the stigma commonly associated with personality disorder – whereas complex PTSD seems to carry less stigma!
Rachel: I would never want to ignore this question. This is what I have spent my working life talking about, learning about and trying to get people to understand.
Complex trauma is an organisation framework that brings together a set of responses that include emotional dysregulation, difficulties around trust in relationships and a fragmented sense of self. It is most often associated with trauma that has occurred in close, care giving relations, especially in childhood. When children are hurt by those that are meant to care they not only experience the trauma itself and the associated violations but they also have no refuge from the fear. In addition they miss out on the safe relationships where children learn about regulation, who they are, and how to build trusting, safe relationships. If you look at Borderline personality disorder against the context of what individuals have experienced many of the symptoms rare about managing unmanageable situations, feelings and experiences.
DD E: In this vein then, would you say taking a trauma-led approach to BPD is a valuable one? As therapies currently tend to take a behavioural approach (I’m thinking DBT and the like).
Rachel: I would say a trauma-led approach should be essential in any approach to working with someone who has received a diagnosis of BPD. I would like to see a much stronger emphasis on trauma around work with these individuals. BPD is often associated with a lot of trauma in relationships both in childhood and adulthood, trauma that has occured at developmentally vulnerable times and from someone in a position of trust. The trauma is not always event based, it can also be about what someone has not received such as with neglect. That is not to say interventions like DBT don’t work but they treat emotional regulations and support alternative coping strategies to coping such as self-harm. I think it is also important to know what has happened to someone so they can make sense of how they are feeling and seeing the world and themselves. More self-compassion is key.
DD E: Are there treatments available to help those affected by trauma. Ive heard of EMDR – is this something that would help traumatisation? Im thinking psychological treatments
DD E: Not an expert here (so may be overstepping, sorry!) but as someone currently going through EMDR it can be really really effective for processing traumatic memories. The way it was described to me is that traumatic memories get “stuck” and cause lasting distress as they haven’t been processed, and EMDR is a way to un-stick them.
DD A: I’m really interested to hear the answer to this too. I found EMDR very helpful and curious to know others’ experiences.
Rachel: EMDR is an exposure based intervention and so is particularly helpful for processing fear based symptoms such as flash-backs and nightmares. It can be helpful for the right person. The shame that is so often attached to trauma, especially interpersonal trauma often takes longer to shift and need time, a safe relationship and the opportunity to explore beliefs about self, others and the world. Survivors of trauma carry a lot of blame and I take a compassion focused approach.
So good to hear about people getting access to trauma-specific interventions. This is so important. EMDR is one of these, glad it was helpful. So many get other aspects treated first i.e. substance use, low mood, self-harm. And it takes so long for someone to ask “what happened to you?”.
DD E: Is EMDR available on the NHS and if so is there a long waiting list? Or even a recommendation of private therapy?
Rachel: EMDR is available in many NHS psychological services especially trauma specific services. What is available and how long the wait will depend on the NHS Health Board. EMDR has a UK Association that can recommend therapists.
DD A: at the end of my CBT sessions my NHS therapist asked if I wanted to try some sessions of EMDR (she was doing a course in it for her job).
DD S: The link one of you shared earlier, about ACEs, listed big traumatic events, like child abuse, violence, etc. But what about ‘normal’ traumas, that almost everyone experiences at some point – e.g. the end of a serious relationship. And then ordinary stressful events – losing your wallet, missing a train, failing an exam – which can feel like a big deal at the time.
What is the difference between stressful life events and trauma? Is it just the size or number that makes them different?
Rachel: Interesting question and one that is often asked. There are a number of ways in which the experience of trauma can affect individuals that can have an impact of better or poorer outcomes. These include the direct impact of the trauma/s, whether the trauma impacts on an individuals ability to cope and whether it impacts on relationships. The impact of stressful life events is often cumulative, little things chip away and impact on resilience. Trauma is often experienced as threatening and leads people to believe that the world is threatening and unsafe place. This can lead people to avoid relationships and experienced hat might help.
Hope: Hi, that is a good question! We tend not to look at traumas as ‘big’ or ‘small’ etc, because as you said, everyone’s experience is different and what feels like a big deal to someone, might not feel like much at all to someone else.
Typically when someone has experienced a traumatic event, there is about a four week period the the trauma taking place and perhaps traumatic symptoms starting to develop. This four week period is important, because as you quite rightly pointed out, it may have felt like a big deal in the moment, but as time goes on you are able to carry about your normal life and it doesn’t really bother you. However, there are perhaps other traumas that happen in your life, that will tend to stick with you a bit more. You may find that you start experiencing flashbacks or nightmares, you might start actively avoiding reminders of the trauma, or feeling like you are constantly on edge or feeling jumpy all the time. If these symptoms start developing in that four-week window and continue to get persistent or make it difficult for you to function in your daily life then you may need to seek additional professional support for this experience.
Hope this answers your question 😊
DD S: Thank you both. Yes, that is useful.
DD E: Do siblings (one male, one female from the same family) react differently to a severe traumatic accident?
DD M: I would say this is all tied up with the culture they are growing up in. Because there are no significant differences for male/female brains
Hope: A good question here and an interesting one! It is difficult to say, are you suggesting here that both the siblings experienced the same trauma? Or maybe one did and one didn’t?
Either way, you can develop PTSD either through directly experiencing an event, or through witnessing an event taking place.
There is evidence to suggest that females are more vulnerable to developing PTSD post-trauma, but there are also a variety of other factors such as poor social support, and previous experiences of trauma.
I’m not sure I can answer your question specifically, as there are a lot of other factors to consider, but it may be the case that siblings from the same family would react differently to a traumatic experience, as they themselves are different as people.
Karen: There is evidence that females tend to be depressed more than males and they tend to be exposed to trauma more often. However, in terms of siblings, and the same event, it would depend very much on the individuals involved as siblings have different genetic make-ups, personalities, support circles and so on.
DD S: I’m interested in your point that trauma might not be ‘an event’. I’ve often imagined that the ongoing experience of growing up, eg, in a violent and unpredictable home, and having no real place of safety, would be much worse than the ‘one-off’ trauma of experiencing a terrorist attack, or another act of violence. Is this what you see in the research? How does continuous and prolonged trauma differ from a one-off event?
Karen: Great point. A ‘one-off’ event is of course extremely stressful but even high levels of stress can be managed if people have developed good self regulation skills and have support. For children and young people, whose brains and stress regulation systems are still developing, ongoing chronic trauma through neglect or abuse or loss can put an intolerable load on a young person who has not yet developed these skills. This continuing stress can actually start to affect the way the brain and other body systems function, making that person potentially more vulnerable to stress, depression and PTSD in the future.
Always important to add, however, that this is not inevitable and people can recover from trauma.
I also wanted to add that living in poverty is traumatic, as is neglect which can feel life threatening to a young person. Of the different types of trauma, a recent meta analysis showed that emotional abuse is more strongly linked to depression than other types of abuse. We tend not to think about the impact of emotional abuse too much but it can be very pervasive and potentially damaging to a child.
DD S: What about if both the imaginary people are adults? I mean, eg, the stress of living in an abusive relationship vs a one-off traumatic event?
Karen: It is very difficult to categorise the effects of trauma. I see what you mean that a one-off traumatic event may present less chronic stress in some cases than ongoing fear-related events (such as an abusive relationship). However, people respond to trauma in different ways that reflect their past, their relationships etc. so for one person something might lead to mental health impacts, where it doesn’t for another person. That said, abusive relationships are particularly toxic due to the constant exposure to fear.
DD I: What research methods do you use? (We are just considering what methods to use in our group)
Karen: It depends really on what your question is 😉 We use survey methods a lot to collect data on variables that are likely to be contributory. Other methods might include stress tests, observations of interactions etc. What specifically are you trying to research?
Hope: In my work I use a mixture of both quantitative approaches (e.g., questionnaires) and qualitative approaches (e.g., interviews). I think using a mixture of both is really helpful when trying to address a topic like mental health and parenting. For example, I had one mum talk to me about some questionnaires I had given her asking about the level of communication she had with her child. The questions asked things like “my child looks at me when I say their name or am talking to them”, “my child does what their told the first time they are asked”, “when I speak I feel like my child is listening”, etc. She said to me during her interview she was concerned about those questions, because her child was autistic. So her child didn’t always listen to her first time, and didn’t always look at her when she was speaking to them, but not because their communication as mother and child was poor, but because of her child’s autism. Something like this wouldn’t have been captured via the questionnaire alone, but was discussed during the interview. So I think it is always beneficial to use both where possible 😊
Karen: To add to this, there are a lot of questionnaires on trauma or Adverse Childhood Experiences (ACES – which you might have heard of). These can be very triggering to some people however so need to be used very cautiously.
DD E: Is there much in the way of support groups for trauma/ACEs? I only know of one!
Rachel: Scotland has a National Trauma Strategy which you can read about on the web. There is a strong drive to get as many people as possible to be trauma informed. Organisations like Health in Mind can run helpful groups.
DD E: I am interested in trauma experiences in different places/cultures. Are some cultures more likely to be protective or induce depression? I was interested in the South African context and someone mentioned before about poverty being traumatic and the UK has a big problem with that.
Hope: Yes, you are correct that lower socioeconomic status can make people more vulnerable to trauma exposure and subsequent PTSD development. This has a lot to do with the context that you live in as well. You may be more at risk to being exposed to dangerous situations. In South Africa, it is an interesting one (I’ll try and not go on forever about it, although I really could!), you’re right that culture plays a significant role. With the parents that I have specifically worked with they were Black African parents, who culturally believed that you dealt with trauma within the family and you did not speak about the trauma as you would bring shame on the family if you did. They also lived in a really unsafe environment where their exposure to trauma was continuous, which was also difficult. In addition, a lot of the South African parents I worked with didn’t really understand what their trauma symptoms were, or didn’t make the connection between their trauma and then having nightmares for example. So you’re right, culture and context has a huge influence.
DD E: Very interesting. So people recognising trauma and that some of their feelings are a result of trauma will help them to cope/recover better?
Hope: It can do in certain cases, yes. It gives you a bit more of a sense of control and an understanding of where these symptoms are coming from.
DD N: That’s all we’ve got time for I’m afraid! Rachel, Hope and Karen, thanks so much for coming and answering our questions, this has been great
Karen: Thank you so much for inviting us. We’ve really been kept on our toes with these insightful questions. It was a real pleasure!
Rachel: It is really important for all of those who have experienced trauma to be given understanding, support and the right access to psychological approaches. Many symptoms are coping strategies that were essential at the time. Survivors of trauma carry so much self blame. they need our compassion not our judgement.
Hope: Thank you so much everyone for all your interesting questions, this has been great 😃
DD C: Thank you so much! I wish we could meet and chat things through properly as this format is really hard to keep up with (especially when my 7 year old daughter had a massive meltdown and needed soothing so I was very late!!)
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was withMorag Allan Campbell, a historian specialising in mental illness in pregnancy and childbirth, particularly in Scotland between 1820 and 1930.
Q&A
Hi Morag!
Morag: Hi, thank you so much for the invitation, I’m very pleased to be joining you here tonight.
I’ve recently finished my PhD in Modern History at the University of St Andrews, and my research focuses on postpartum mental illness in nineteenth century and early twentieth century Scotland, looking not only at what doctors thought and what treatment they used, but also at what families and communities understood and how they dealt with mental illness during pregnancy and following childbirth.
Depression Detectives member I (DD I): For those that are not quite sure (like me who just looked this up!), Morag looked at the years 1820-1930.
Morag used records from the chartered asylums at Montrose and Dundee, court and prison records, and newspaper accounts, to explore how childbearing-related mental illness was recognised, accepted and supported by families, neighbours, friends and authorities.
DD N: I’m interested in the family and community aspect – were people supportive of mothers experiencing mental illness in that time or not so much?
Morag: That varied a lot from case to case, but, on the whole, yes, it seemed to be something that families and communities seemed to expect. Most of my work is based on asylum records and it’s difficult to know much about what they did before women were admitted, but we can piece together stories of how families tried their best to look after women until they could no longer cope.
DD S: You looked partly at how attitudes and treatment differed by class and social group. Could you tell us a bit about what you found out?
Morag: They looked for different behaviours and values in private and pauper patients – willingness to work was seen in pauper patients as a sign of recovery, while the private patients exhibited self control and engaged themselves in genteel activities. They foregrounded different attributes in the patients also. But basically, they judged the poorer patients according to middle class values, which were often difficult or impossible for them to achieve.
DD A: Your thesis sounds really interesting Morag. Congratulations for completing! I’m interested in how how mental health issues would be diagnosed in women after childbirth before the NHS. Did they have midwives? Was there much aftercare? Would they go to a doctor?
Morag: Thank you! Yes, there would be midwives, but they weren’t like professionals at that time. Families would usually begin to notice symptoms, changes in behaviour etc, and most would just struggle on until the woman’s condition improved – most of this is undocumented, so it’s hard to know what really went on. Doctors would be called in if they really couldn’t cope. There wasn’t really any official after care.
DD C: Have you looked at comparisons/ differences between what is diagnosed as postnatal depression or postnatal psychosis today, and what women experienced in the period you studied?
Morag: Yes – there are definite similarities across the different time periods, but in the nineteenth century, the symptoms reported were different – one researcher who did a comparison said that nineteenth century symptoms were ‘more florid’. But the condition tended to be measured much more in moral terms than we would do today.
DD C: What does this mean, in more moral terms? What kind of effects did being unwell have for women?
Morag: They defined mental illness in terms of adherence to appropriate norms of behaviour and assumptions about what was appropriate for each gender.
DD S: What does ‘more florid’ mean?
Morag: I think he meant more extravagant and varied
DD N: Would that mean some people who were diagnosed as mentally ill would be considered not to be unwell by today’s standards? Or is it more that the effects on behaviour were caused by mental illness, but the behaviour changes were what was considered important?
Morag: Good question! What we regard as mental illness differs according to time, culture and society – so yes, it’s a bit of both.
DD I: How did people get out of asylums?
Morag: They were discharged when doctors felt they were fit to leave, and this was usually negotiated with the family. Often, at the asylums I was looking at, they would be sent home on a trial basis. There’s lots of stories about people being ‘put away’ for years, but asylum care was actually quite expensive. I came across more incidences of families trying to get their family members discharged before the doctor thought they were cured. Generally, I felt the doctors were really trying their best to help their patients and were often deeply saddened if they felt the patient had left the asylum before they were restored to health.
DD S: You studied the period from 1820 to 1930. How did attitudes and experiences change over that time?
Morag: Early in the nineteenth century, the dominant idea and treatment was what they called ‘moral treatment’ – it was a new age for treatment of the mentally ill, and they believed they could cure mental illness with the right treatment. Moral treatment revolved around middle class family values and the importance of work in maintaining good mental health. The 1800s saw a big rise in asylum care – with the intention of cure – but by the end of the century, ideas had gone over much more to the idea of the hereditary nature of madness, and they were less confident about cure.
In terms of postnatal mental health, in the 1800s it was all about what they called ‘puerperal insanity’ – they saw this as a distinct condition that they could cure – this also went out of favour by the end of the century, and in the early 20C the diagnosis disappeared. They no longer regarded it as a separate condition and in fact postnatal mental illness also became invisible in the first half of the 20C (making it very difficult to research!).
DD S: “the importance of work in maintaining good mental health”. Sounds a bit like the workhouse! Were women forced to scrub laundry and so on?
“Moral treatment”, were they being read extracts from the bible and things like that?
Morag: That’s an interesting comparison! The work ethic was very much part of the treatment, so yes, they were made to work, but only when they were fit to do so, and they did various things. The doctors thought that work occupied the mind and kept dark thoughts at bay. Women did work in the laundry, but also in spinning and weaving, and helping out on the wards. There were also cases of women being employed as nurses/attendants after they were discharged. Later in the century, most asylums would usually have farms, and patients would work in these to grow and produce food, for consumption in the asylum and outwith. It was seen as a collective thing, and many of the patients took pride in it. I expect they were read lots of things out of the bible (Sunday worship was a big thing, but then it was outside of the asylum too at that time); but moral treatment really meant training the patient to behave according to strict moral values, and recovering the patient’s reason through encouraging appropriate behaviours and attitudes.
DD S: What did Victorians think the *causes* of postnatal depression were? And what kind of treatments did they use?
Morag: There was lots of debate about this, and ideas about what actually caused it varied enormously. But at the root of it, they believed that women’s reproductive organs and cycles were pretty much the cause of all a woman’s mental health problems, and puberty, childbirth and menopause were seen as particularly dangerous times.
Having said that, treatment was pretty much the same for any patient, as they had little useful medication to give. Treatment usually started with the bowels – they were very keen on purging! There was also some bleeding and cupping (blistering). But mostly, they concentrated on giving women a good diet and a rest. Many of the women I looked at were living in poverty, and their stay in the asylum gave them a regular decent diet, and they would also get treatment for ongoing health conditions, such as piles. Improving the patient’s physical health had positive consequences for their mental health.
DD S: So they thought of what we would now call PND as a completely separate thing from other forms of depression?
Morag: Yes, though again there was much debate about this, and not all doctors agreed that it was separate.
DD N: You mentioned asylum care was expensive – how were women living in poverty/their families paying for it? or was it ever subsidised?
DD S: In Scotland, most asylum care was provided by large charitable institutions, funded through public donations and fees. There were very few private asylums in Scotland, and the big asylums catered for private and public patients. The fees for the private patients were paid by their families, and the pauper (public) patients had their fees paid for by the parish they belonged to – local authorities were basically church-based.
DD N: And that’s all we’ve got time for! Thanks so much for coming Morag, this has been super interesting
Morag: I hope all that made sense – those were some really good questions! 😃
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with Daniel Smith, a psychiatrist from the University of Edinburgh who is part of a sleep research project called SCRAMS (Sleep, circadian rhythms and mental health in schools). We were also joined by Heather Whalley, who works with Daniel on SCRAMS and led our Q&A on brain imaging.
Q&A
Hi Daniel!
Daniel: Evening everyone. I’m a psychiatrist and researcher with a special interest in bipolar disorder. My interest in the connection between disturbed sleep/circadian rhythms and mood disorders includes research on the genetic overlap, research on sleep and depression in young people and more recently an interest in ‘chronotherapies’ such as bright light therapy for bipolar depression
Depression Detectives member N (DD N): Could you tell us what the genetic overlap is?
Daniel: This is about common genetic variants that slightly increase our risk of sleep disruption also being associated with increased risk of mood disorders. It’s due to many of these variants combined, rather than single genes
DD E: So change in sleep pattern can trigger depression in bipolar?
Daniel: Yes – sleep deprivation is a common trigger for mania. I should add that this is also about disrupted rhythms of rest/activity, not just sleep per se
There is some evidence that genetic factors that predispose us to sleep problems are shared with genetic factors for depression and bipolar disorder, and traits such as mood instability
DD E: Oh interesting so it plays a role in the highs and lows of mood?
Daniel: I think anyone will have changes in their mood the day after a bad night’s sleep but people who are vulnerable to depression and bipolar disorder are probably more sensitive to this and less able to compensate. A classic example is that crossing time-zones in air travel can really disrupt our circadian rhythms (and gives most people jet lag) but people with bipolar disorder can become much more unwell
DD E: does melatonin treatment help with bipolar the same way some people use it for jet lag?
Daniel: The evidence for melatonin in bipolar disorder is pretty weak – it sees that people with bipolar disorder need a more robust way to regulate their sleep patterns
DD S: I’ve heard that sleep deprivation can help depression. For example see this article. My question is, does this apply to everyone, or to a subgroup of people with depression – notably, does it apply only to people who oversleep when depressed? And is there consensus on what ‘sleep deprivation for depression treatment’ should consist of e.g. one 24h without sleep? A longer period with an hour or two less each night? It seems like it would be worth trying…but are there risks? (if you’re undiagnosed bipolar I would think this could trigger mania, for instance)
Daniel: The idea of using sleep deprivation as a treatment for severe depression has been around a long time and it’s good to see some more recent studies. Overall, it can be effective for some people but I think it’s fair to say that the effects are often short-lived and this is not an easy treatment to deliver (it needs lots of staff time and resources, for example)
DD E: staff time to keep the patients awake? And can people do sleep therapy by themselves?
Daniel: So it need quite intensive nursing to ensure sleep deprivation
DD N: Sleep is often mentioned as a symptom/factor in depression, but it seems people go either towards sleeping way more than usual or struggling to sleep at all. Is there any indication as to why people experience different effects on their sleep?
Daniel: In general (but not always) depression is associated with worse sleep and bipolar depression with more sleep
Heather: That’s a really good point, and some of the difficulties in depression research (I work with Daniel) – people experience different and sometimes opposite symptoms, like increased or decreased sleep, and increased or decreased weight for example. We are only just starting to tease these things apart.
DD S: Do you think it’s because actually people are experiencing different types of depression? Or that different people respond differently to the same thing? Or that there’s almost a biological or behavioural coin toss somewhere, and the same person could go either way?
Daniel: Very good question – obviously it’s complicated, mostly because depression is not a single disorder – more likely a collection of slightly different disorders with some common symptoms
Heather: I’d like to say we know, but we don’t as far as I’m aware. There have been genetic studies trying to tease these things apart (to see if these might be different subtypes based on the type and direction of symptoms, and different underlying causes ), but we’ve only recently had sample sizes to do this kind of analysis, and I’m not aware of anything convincing as yet, tho Daniel might know more….
DD S: How would you even study that then? What kind of experiments would you do?
Heather: there are v big studies like one called UK Biobank which has genetic data and some information on depressive symptoms, but often because of the scale (0.5 million people) some of the nuanced symptom data is lost – but its a place to start…So essentially looking to see what large datasets there are with the right sort of information.
DD C: Could you tell us a bit more about how chronotherapy works? And is this suitable only for some people or for everyone who has depression and has sleep problems?
Daniel: Light boxes in the winter can help most people with mild seasonal depression or lack of energy in winter and bright light in the morning is now being seriously investigated for bipolar depression
DD A: Hi Daniel, is there much research about starting school at a later time for teenaged children because they are unable to sleep long enough when school starts at 9am?
Daniel: Our SCRAMS group are reviewing the literature on this but overall it looks likely that even a small delay in schools start times is beneficial for teenagers, who are not programmed to wake up properly until about 11am
DD S: Teenage me feels vindicated here!
DD C: Not just teenage me. All my life I’ve had this problem. I wonder if it’s related to poor quality sleep in adulthood, say because of sleep apnoea?
Daniel: yes – all sorts of causes
Heather: There is increasing research here I think, and discussions not just about later start times, but thinking about the content/subjects for the earliest lessons
Daniel: Also, we shouldn’t be expecting teenagers to go to sleep at 9 or 10pm when their body is telling them 11pm or midnight
DD N: This makes me wonder whether teenagers who are living in situations without artificial light have the same difference in sleep schedule as teenagers living in electric-lit houses!
Daniel: Too much light at night for teenagers is a very bad thing!
DD N: Is too much light at night worse for teenagers than adults?
Daniel: Yes – I think this is very likely true
Heather: interesting 🤔!
Heather: Someone posted during the week about if we know what comes first, the sleep problems, or the depression. Do we have any info here Daniel?
Daniel: Not sure – sleep problems are a trigger and a symptom, so hard to untangle this
DD N: Do you have any thoughts on what kind of research would be needed to figure it out?
Daniel: I think we need very carefully designed prospective follow up studies of large numbers of young people and collecting objective data on sleep and mood to see what comes first and then what happens after a depressive episode
DD S: From a discussion thread in this group, it seemed like a lot of us were natural ‘owls’. Is there any research on chronotypes and depression? Are naturally late-rising people more prone to depression? (Either because there is some connection between the causes, or because late-rising people are more likely to experience sleep deprivation, in ‘9-5’ jobs/schools?).
Daniel: Sorry to say that night owls are more likely to have a range of adverse health outcomes, including more depression. Evening chronotype makes it more likely to experience circadian disruption
DD S: Do we know why the worse health outcomes?
Daniel: Because the circadian system controls all of our biology – from eating to immune response to hormone release – it affects all sorts of functions
DD S: So you’re saying evening people have worse health outcomes because their circadian rhythms are more likely to be disrupted. But is that BECAUSE school and office hours, etc, are set to suit morning people? ie it’s the social setting that causes the health outcomes effects, rather than the chronotype per se?
Daniel: I think some people cope well with our (very unnatural) 24 hour modern living – these people are more often morning larks, so yes modern society suits larks.
DD S: I’m now wondering if there’s any research looking at this during the pandemic? I mean, a lot of people have been working from home, and more easily able to have a sleep schedule that suits them. Have owls found this has improved some aspects of their health?
(I realise it’s probably difficult to separate the sleep schedule from everything else that’s been going on….)
Daniel: I’ve seen a fair bit on sleep during the pandemic, eg, everyone is having more vivid dreams (because they are sleeping more naturally without alarm clocks and are more likely to wake up during a dream)
DD S: We’ll that is fascinating! I’d always assumed we naturally wake up at the end of a dream. Is that not the case?
Daniel: we dream about 5-6 times per night, during REM sleep which cycles veery 90 minutes but we dream more at the end of the night
DD S: And our brain doesn’t ‘wait’ to wake us up after the dream has finished? But just kind of wakes us up as it’s still going on? (Now I’ve typed that, I’m wondering what it would mean to finish a dream. It’s not like it’s a film, with a narrative arc…)
Daniel: it’s just that sleep becomes lighter as the night progresses and we are more likely to wake towards the morning
DD S: What wakes us then? If it’s not the dreaming brain? Who/what decides it’s time to wake?
Daniel: It’s a natural biological cycle of deep and light sleep that recurs 6 times per night
DD S: hence waking between 3 and 4 am being quite common?
DD C: Is the chronotype completely fixed or could a night owl turn into a lark?
Daniel: young people are morning larks, then teenagers are evening owls, then older people are morning larks again, so it changes through life and can be modified by training
DD A: My children (8 and 4) are natural night owls, like me. They will sleep reliably around 10pm and struggle to wake up. Should/could I be actively training them to sleep and wake earlier?
Daniel: I don’t think so – probably best to respect their natural rhythms as far as possible – they will change as they get older
DD E: People who regularly change their sleep pattern, e.g. to do day and night shifts on rota, are they more likely to get mental health problems doing that?
Daniel: yes, I think it has been shown to be not good for health generally, fighting natural circadian rhythms. In general shift work is very bad for our long term mental health and people with mood disorders should probably avoid shift work if possible
DD L: Is the quality of sleep different in people with depression? E.g., less deep sleep.
Daniel: In general yes – less deep sleep, more waking etc
DD E: Reading your answer on bipolar sleeping later in the morning resonates with me and I find I can go to sleep fairly easily in quite a good settled mood, but wake in the morning feeling down and depressed. Is this typical for bipolar disorder?
DD M: I’m not bipolar but can also experience this
Daniel: Yes – in bipolar depression (and more severe unipolar depression) people have more diurnal variation in mood , usually feeling much worse in the mornign and better as the day goes on
DD M: how would one determine ‘more severe unipolar depression’ please?
Daniel: Just more severe symptoms, more debilitating fatigue, loss of appetite, weight loss, preoccupations with dying etc
DD E: During times of depression are dreams on more of a depressed theme?
Daniel: I’m not a Freudian (much) but I think that could be true for many people!
DD M: lots of mine are anxiety dreams. If I remember them
DD L: Does lack of sleep play a role in the development of post natal depression?
Daniel: Yes indeed – an important factor among many
DD E: One more question – does depression medication affect quality of sleep in a therapeutic way? Or does it interfere/block sleep quality
Daniel: It depends on the medication I think – some drugs, eg, benzodiazepines do provide good sleep and others, eg, SSRIs might help sleep but it can be a bit more superficial/less satisfying
DD C: I can certainly affirm that SSRIs gave me incredibly lucid dreams, especially ones where I was flying. I was also often aware in the dream that I was in fact dreaming and could to some extent take control eg I think I’ll fly over there now. Unfortunately it was shortly afterwards that I would wake up.
DD N: Do you think there are any major gaps in the research in this area?
Daniel: In general I think psychiatry has not paid enough attention to how manipulating sleep patterns can be therapeutic, eg, using light and other chronotherapies – part of the reason is that there is very little money in this for drug companies
DD S: Ooo, I had one more question. I find that if I walk outdoors each day (my usual form of exercise), then my sleep is much better. We know that exercise is good for depression. But do we know if the exercise directly helps the depression? Or is it because the exercise makes your sleep better, and that helps with the depression?
Daniel: My strong view (as yet unproven) is that outdoor exercise helps our mental health via an indirect effect on better sleep caused by morning light exposure
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with Charlotte Huggins, a researcher with Generation Scotland.
Charlotte is currently working on a project called TeenCovidLife, examining how the well-being of young people age 12 to 17 in Scotland has been affected by the COVID-19 pandemic. If you’re aged 12-17 and living in Scotland, you can get involved here.
Q&A
Hi Charlotte!
Charlotte: Evening all! I’m Charlotte, a researcher with Generation Scotland. I work on the impact of the pandemic on mental health, particularly in teens. I’m also really interested in mental health in autism, and the role of emotion. Before the pandemic, I also worked in Japan for a couple of months! Now I’m working at University of Edinburgh.
Depression Detectives member C (DD C): We had a bit of a discussion in our group about what’s the worst for kids in Covid-times, and some felt the rhetorics around “falling behind” education-wise is impacting kids more than anything else these days. Is that something you’ve found in your studies?
Charlotte: That’s an interesting point! We don’t have data on that exactly, but I do personally think the relentless doom-and-gloom around young people’s education might be counter-productive. After all, especially for teenagers, the standards they should be ‘at’ at every stage are something we invented! I think instead of frightening young people with prophecising, we should focus on making positive changes to support their education and mental health in these difficult times.
DD I: From the main group:
Are there links between autistic traits and depression (and/or autoimmune conditions and/or somatic conditions)? Autism being the particular point of interest.
Charlotte: I can’t speak to autoimmune conditions/somatic conditions (not something I’ve ever looked at!) but there are definitely associations between autistic traits and depression. Autistic people have much higher rates of anxiety and depression compared to non-autistic people. And in non-autistic people, higher autistic traits is likewise associated with mental health difficulties.
DD C: Do you know anything about reasons for these higher rates? For example, does it have something to do with how the mind is wired, or how much difficulty people with autism experience in daily life through stigma, etc.?
DD S: And do we know anything about whether that is something intrinsic to autism, or does it come from the difficulty of navigating the neurotypical world as an autistic person? I don’t even know how you would do research to try to separate those two things!
DD M: My guess would be that society disables autistic people. Everything is geared towards neurotypicals.
It’s still called a disorder, which in itself is stigmatising. I think that professionals in particular need to listen to autistic people
Charlotte: I personally think it’s more to do with being an autistic person in a neurotypical world! Autistic people experience much lower rates of employment and education, suffer from lower self-esteem, and often have difficulties forming and maintaining good social relationships (which are a great protective factor against mental ill health). If the world was made more accessible to autistic people (including improving attitudes towards and understanding of autistic people), I believe much of these issues would improve.
DD S: What are the ‘headline findings’ that Generation Scotland has been seeing in relation to the pandemic and mental health?
Charlotte: This is some analysis I’ve not quite finished yet (so please take with a grain of salt!), but we’ve been finding a definite increase in depressive symptoms during the strictest lockdown measures, which improve as lockdown measures ease. However, anxiety seems to have risen in February, which I wonder if relates to uncertainty around the new variants and vaccine rollout. I’m doing some really exciting stuff with other UK cohorts to find out exactly more about how it’s changed over time, and how it compares to pre-pandemic.
DD C: Really interesting. I’m not very familiar with cohort studies. Do you take “random” things into account such as, say, the weather/time of the year (my mental health is the worst in February)?
Charlotte: It depends on the type of analysis being done! Since we have such big data, many people work on it, and different types of questions require different types of analyses to answer. I’ve personally never used weather/time of year (I imagine pulling in all that data would be difficult) but I’m sure there’d be some fascinating analysis to do there.
DD S: Something came out recently that seemed to show that depression was twice as as high as normal in the first few months of this year. Would your research agree with that? If yes, does it look like people who have previously experienced depression all getting depressed at once? Or is it new people getting depressed?
Charlotte: I’m not sure! We’re working on analysis that is looking at this change over time more closely, but it’s not quite ready yet, so I don’t want to jump the gun. I’d hazard a guess that there was an increase at the start of this year, between the gloomy weather, the increased restrictions, and the fatigue of almost a year under the pandemic. But whether depression rates have doubled, I wouldn’t be able to say!
DD M: What do you think are the differences between children/young people and adults when it comes to how they are affected by the pandemic? Is there anything additional to look at here that might be different?
DD E: I’m wonder if there was any distress apparent in the teens of either Covid or lockdown and the disruption to their education?
Charlotte: I think for young people, the impact on schooling is the biggest issue. Many older teens are experiencing a lot of uncertainty and stress about how this will affect their future job prospects and getting into university. And just getting the placement often isn’t the end of the issues – making friends, forming long-term relationships, settling into your adult life…all of that becomes more difficult when done remotely. I think people in transitionary life periods are probably experiencing very particular challenges.
DD M: Some autistic people might have felt relieved by some of the restrictions during the pandemic. Is there anything we can take from this to aid mental health going forward?
Charlotte: That’s definitely something I’ve seen as well! I think the changes we’ve made in response to the pandemic can be wonderful for autistic people (and many other people beside!) – such as more options for remote working/schooling and reduced crowding in public places. I think moving forward, it would be great to keep these accessibility options in place. We’ve proven now that it is possible to make these changes, and a lot of places now have infrastructure to do so!
DD E: Did you find it more onerous to collect data during lockdowns or was it actually easier to find participants because of lockdowns?
Charlotte: The CovidLife projects (Check out this link for more detail: https://www.ed.ac.uk/…/generation…/covidlife-volunteers) have seen really good returns! I think particularly for Covid-related research, people are keen to participate and have their voice heard.
For projects that can’t be done online, though, it gets much difficult. Just before the first lockdown in March, I was planning a study about interoception (the ability to identify your own bodily sensations). This would have involved me passing the same objects back and forth to participants over the course of an hour! As you can imagine, that never quite came to fruition 😄
DD C: I heard that teenagers’ eating disorders increased a lot during Covid. Have you seen a reduction in this now, since there are less restrictions on kids’ sports and they can go back to school?
DD N: Potentially might be linked to the control element of EDs? With so little control over all the external factors of the pandemic.
DD M: my thoughts too
DD S: Can I just check about how Generation Scotland works. You have a load of people signed up, and you ask them lots of questions at the beginning, and you get access to their medical records? And you also send them more questionnaires from time to time? And then you can basically ask questions of all this data? Like, you could ask it ‘Are people who live near the sea more likely to get depression?” And if they are, you’ve found something out.
And I know the list must be super-long, but could you give us an idea of the kind of data you have about people?
DD E: My question is firstly how you collate your data and when you have gathered it in how you design the data? Hope that makes sense.
Charlotte: Yes, Generation Scotland is a cohort study, so a lot of it is about collecting detailed data. We have some of the most detailed data on our participants in the UK! When GenScot started (back in 2006, while I was preoccupied with being in primary school), participants took part in a clinic visit which involved taking a lot of detailed measurements, and provide genetic samples for analysis. We also link to NHS data. The exciting thing about GenScot is that we’re a family study – meaning people join up as part of families, so we can link their genetic data together. We even have neuroimaging data!
This year, we’re planning a new wave of recruitment. This time, the initial measurements will be done completely online, in our new system. Participants will be sent a kit in the post so they can submit a saliva sample to us for genetic testing.
And yes, the benefit of having such a big bank of data to work with is that we can address many different research questions. Other researchers can apply to use our data (without any identifying data of course!) and answer research questions. There are over 250 publications in academic journals using Generation Scotland data. Here’s a great link if you want to see a bit more: https://www.ed.ac.uk/generation-scotland/what-found
DD S: So what kind of data do you have about people? What questions do you ask them?
I mean, I’m assuming postcode, parents occupations, obv all these samples, but do you give them personality tests? IQ tests? Do you ask them about their hobbies? Pastimes? Diets? Sexual activities? Jobs?
Charlotte: We have a lot of this! We have personality data, cognitive ability data, diet and exercise habit, employment, health history and health behaviours, I don’t think we have data about sexual activity or past-times though.
DD I: We hear alot about young people and social media. Did this come up in your study? I guess it has positives and negatives during lockdown?
Charlotte: We didn’t spend many questions on social media in TeenCovidLife, unfortunately! We didn’t want the survey to be too long. In the first lockdown, about 54% of teens said their social media use had increased. But, after lockdown ease, 50% said they used it less than during lockdown!
DD C: Do you check whether self-reports tie up with other measurements?
DD E: I came across a graphics timeline (link) on Twitter which was amazing.
How many hours and people would be involved in that?
Charlotte: It’s fantastic isn’t it! Amazingly, the majority of that was done by just one of my colleagues. I will definitely pass on your appreciation to her 🙂
DD N: And that’s all we’ve got time for! Thanks so much again for coming Charlotte, this has been really great
DD E: Thank you Charlotte for a very interesting Q&A. Let’s hope we all don’t have anymore lockdowns to contend with even if researchers produce very interesting facts. 😊
Charlotte: Thank you so much! Would it be at all cheeky if I plugged the ongoing work we’re doing for TeenCovidLife?
DD S: Please go ahead!
Charlotte: We’re currently collecting data for our next sweep of TeenCovidLife! If you have or know a 12 to 17 year old living in Scotland, we’d appreciate it immensely if you passed the word! The survey can be accessed here. Questions about exams, school, mental health, and how pets help us in the pandemic (the latter I’m very excited to get data on)
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with Mark James Adams, a statistical geneticist from the University of Edinburgh.
Q&A
Hi Mark!
Mark: Hi, everyone. I’m a researcher in the psychiatry department at the University of Edinburgh. My background is in computing, genetics, and psychology. I mostly work with population health datasets doing genome-wide association studies (abbreviated “GWAS”), where I look across the whole genome to find parts of our DNA that increase or decrease the risk of having depression.
Depression Detectives member E (DD E): Can the symptoms of depression lie dormant, for eg teens/adulthood then manifest at say 40 due to change of life and hormonal imbalance?
Mark: Yes, we do see differences like that. Some people seem to be at risk for having depression but have not yet experienced a life event stressful enough. For example, childbirth is a very stressful time for many people, especially mothers.
Here is a figure from a paper by one of our researchers showing different trajectories of depressive symptoms from adolescence to adulthood. The higher the number in the figure, the more depression symptoms a person has, and each line represents a different trajectory that the burden of symptoms can take.
DD N: Do most people who experience depression fall into one of the groups on the graph?
Mark: Yes, the “stable low” trajectory is the most common, followed by the “early-adult onset” type. The “childhood persistent” was the least common.
DD M: That childbirth can be a very stressful time is in itself rather depressing!
DD S: I feel like becoming a parent is the really stressful thing…!
DD M: both? 🤷♀️
DD S: Yes, both I guess. And on top of childbirth itself, the hormone changes are huge. But becoming a parent is an earthquake in your life that never goes away, if you know what I mean.
DD I: Being a parent means you are ‘always on duty’. No longer can you just go off for a walk for example.
DD A: Can you tell us about the kind of projects you’re working on at the moment?
Mark: My big project at the moment is part of the Psychiatric Genomics Consortium to do a large genetic study of depression. https://www.med.unc.edu/pgc/
One thing we have learned about genetics for depression is that each part of your DNA makes only a tiny contribution to making you vulnerable or protecting you, so it takes data from a very large number of people to identify those differences. In the study I am working on now, we are combining data from 3.5 million people from all across the world.
My other main project is a genetic study of symptoms of depression. Most of our data are just based on yes/no assessments of depression, so I want to see if there are genetic and environmental factors that influence specific symptoms. I have found that there is a genetic difference between somatic symptoms (like fatigue or changes in appetite or sleep) and psychological symptoms (like low mood or lack of interest in pleasurable activities).
DD S: That’s interesting. What portion of the risk is genetic?
Mark: About 30% of the differences between people is genetic, and about 10% is from differences between family environments.
DD S: I don’t know if this is within your remit to know, but how does that compare to other risks? I know we were talking in the group the other day about how big an influence poverty and precarity are. They seem much bigger than I had quite realised.
Mark: Yes, the genetic portion of depression is low compared to other psychiatric traits like schizophrenia or bipolar disorder. In terms of genetic risk, depression is more like heart disease or diabetes. I think the environment is hugely important and we are still trying to find good ways to measure it, since what each person finds stressful can be very different.
DD N: How are the environmental factors measured at the moment? Or have they just not been studied much?
Mark: We collect lots of data on childhood experiences, strength of family connections, community involvement. This is from asking people about their lives, but we also pull in information based on where people live (for example, is there a lot of green space around).
DD S: So is it you, or colleagues, who analyses the rest of that data? I mean, if we wanted to find out if living near a chip shop affected your chance of getting depression, how easy or hard would that be to do? (Living near a chip shop is just a random example off the top of my head…)
DD I: Yes, if we chose a question like that, Mark Adams is the first person I would turn to!
DD S: Awesome. In that case, I have a lot more questions I’d like to ask. Can Mark come again?:-)
DD N: Really interesting about different symptoms having different genetic causes! In Stella’s Q&A she talked about the idea that maybe depression might not be all one illness but a group of different things, do you think that different symptoms having different genetic causes is evidence for that being true?
Mark: Yes, I agree with Stella. While there does seem to be something common genetically across all types of depression, there are probably differences that drive how depression is expressed as different symptoms.
DD A: Can you tell us what the GWAS is (in simple terms 🙂)
Mark: In every part of your DNA, you have two copies of each variant or gene, one from each parent. What we do is we pick one of the variants as a baseline, and then count how many copies of the other variant each person has. So for a simple 1 letter change in your DNA, there are usually two alternative variants, such as A and C. So the four genotypes are AA, AC, CA, and CC. If “A” is the baseline, then we count how many “C”s each person has (which will be either 0, 1 or 2). We then run a statistical test (called a “logistic regression”) that checks if people with more “C”s are more likely to be depression. We do this test for several million places in the genome and find which ones are robustly associated with depression.
DD S: If the genetic risk is relatively small, compared to other factors, why study it? Why not put all our resources towards, for example, relieving poverty?
Mark: There are a few reasons. One is just to understand the biology of depression. Even if the ultimate cause is in the environment, it’s the ultimate impact is in the body (how the brain reacts and overcomes stress, for instance).
Another main reason has to do with understanding causality. Did the poverty cause the depression, or did the depression cause job loss or breakdowns in relationships that resulted in poverty? With genetics, we know that the causal arrow always has to flow from DNA → Depression. We can use this to identify modifiable behaviors that can help alleviate depression. For example, this type of analysis was used to show that exercise really does help alleviate depression rather than the connection just being that people or aren’t depressed exercise more.
DD I: So maybe if we understand the biology, we might be able to intervene? (e.g. new drugs to treat or prevent depression) is that what you mean Mark?
DD S: Thanks Mark. That makes sense. But can you explain a bit more what you mean when you say this kind of analysis was used to show that exercise does alleviate, rather than depressed people exercising less?
Mark: The type of analysis is called “Mendelian randomisation” There is a good short Youtube video on it: The type of analysis is called “Mendelian randomisation” There is a good short Youtube video on it: https://www.youtube.com/watch?v=LoTgfGotaQ4
DD M: What is it hoped these data might be useful for deriving?
Mark: I hope the data can contribute to finding treatments It would be useful to know ahead of time whether a person is more likely to respond to talking therapy or medication, for instance.
DD N: Is the difference between someone responding better to medication or better to talking therapy something you can see in the data currently?
Mark: We’re still looking into this. The limitation we are currently are having with our analysis is getting good data on talking therapy and how people respond to it. This is easier with medication since we can look directly at prescribing records to see if people are switching from one medication to another, or not filling their full course of prescriptions.
In some cases it might not be that the medication wasn’t working, but that the side effects were intolerable. So we hope to understand this better.
DD I: In the group it was discussed that people may move off medication and onto talking therapy (or something else) that they pay for privately.
Mark: I’m very thankful to this group for that insight. It will help our research tremendously.
DD S: Another tricky question. Are there any downsides to finding these genes? I mean, is it possible that in a future dystopia people selectively abort babies with depression genes? Or people with depression genes get denied health insurance, or whatever?
Mark: I’m much more concerned about implications for health insurance than designer babies!
One thing we know about genes is that they have influence many processes in the body. So tinkering with depression might have other consequences that we don’t know about yet.
The International Society of Psychiatric Genetics recently made a statement on the ethics of embryo screening: https://ispg.net/ethics-statement/
DD S: Like maybe the depression genes are useful for some things? Like sickle cell anaemia protecting people against malaria…
Mark: Yes, that’s what I’m thinking about. The genes can probably have a positive effect as part of the stress response. For example, rumination can be good if it helps you make a better decision or get out of a bad situation
DD S: So they remain in the population, because they are useful in small amounts, or certain circumstances. But if you have too many of them they can cause problems.
DD E: There is exciting news of a new DATAMIND national research hub being led by researchers/scientists based in England. How will this impact on MHSUs /researchers/scientists based in Scotland.
Mark: I hope DATAMIND helps Scottish researchers use data from England, where this type of project will have more of an impact since their data come from so many places. In Scotland everyone has a single unique identifier (called a Community Health Index number) that makes it easier to link our research participants’ data with their health records.
The background to efforts like DATAMIND is that the UK has a very long and rich history of health research studies where the same group of people are followed up over time. These started with birth cohorts in the 1940s and subsequent decades, which were set up to study health and social mobility. There is a lovely book about this history called “The Life Project” by Helen Pearson. https://helenpearson.info/book/the-life-project/
While these studies were hugely important, for decades they struggled with funding. It has only been in the last 10 years or so that their value has been widely recognised. DATAMIND is an effort to build on these research cohorts.
A similar project to see what these kinds of efforts are all about is Catalogue of Mental Health Measures. These research cohorts can look impenetrable from the outside, so one of the biggest barriers to using them is just being able to quickly see what kind of data they contain and to see how they can be used together (for example, I work with the Generation Scotland data set and it is useful to be able to see what other studies have similar measures of depression) https://www.cataloguementalhealth.ac.uk/
This catalogue is very useful for researchers, but my hope is that projects like DATAMIND can turn these resources into a dialogue between study participants, researchers, and the public. In Scotland we are fortunate that it is a lot easier to link between different data sets since, for example, we only have one NHS authority. I’m looking forward to DATAMIND so that we can also better use data from the other nations.
DD N: That’s all we’ve got time for! Thanks so much Mark, this has been really interesting!
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with Andrew McIntosh, a psychiatrist from the University of Edinburgh.
Hi Andrew!
Andrew: Hello everyone. My name is Andrew McIntosh. I’m a professor of psychiatry from the University of Edinburgh and an NHS Psychiatrist in the Royal Edinburgh Hospital. I’m happy to answer any questions you have about treatments for depression. I’ll be here from 9pm until 10pm
Depression Detectives member E (DD E): I would like to ask you about the long term effects of psychotropic medication (lithium and amitriptyline), by which I mean 3 decades or more?
DD A: My question is similar to E’s. What does current research say about patients using an SSRI like Sertraline long term? >3 years.
Andrew: Not very much. The side effects of SSRIs are thought to be greatest at the very start of treatment and with every increase in dose. You tend to break them down more effectively over time, as your liver tries to eliminate them.
As you age however, other illnesses may develop that impact how you deal with the SSRIs. These illnesses (e.g. of the kidney) can mean that the blood levels of SSRIs rise over time and you might get worse side effects whilst remaining on the same dose.
There are long term side effects from lithium with continued use. There are 2 in particular – hypothyroidism and diabetes insipidus.
Hypothyroidism, a common condition is where the thyroid doesn’t produce enough thyroxine. It can be treated by giving thyroxine in a tablet every day. Not ideal, but that’s what many people choose to do. Diabetes insipidus is a condition where the kidneys find it progressively difficult to concentrate your urine. It can be quite disabling and can lead to people drinking and urinating many many times a day. It can’t currently be reversed.
DD M: that’s a bit of a bugger considering I’ve been taking SSRIs (and a few years of SNRI in the middle) for over 20 yrs 😬
DD A: So does that mean you will eventually need higher and higher doses to get the same effect?
Andrew: That could be the case. However (and sorry to complicate this) but the levels of SSRI in your blood aren’t a very good indicator of your response. So the link between dose over time and your response to the treatment isn’t very clear and differs between people
DD M: That’s really interesting.
Andrew: I think so too. If it were as simple as a lack of serotonin, it should be more straightforward. In practice, research suggests that its your brain adaptation to the SSRI that leads to the treatment response. So its fascinating, but there’s still much we don’t know
DD C: Would you be able to explain a bit more what it means that your brain adapts to the SSRIs?
Andrew: I’ve just see your comment. It’s really interesting- after a week or two of treatment, your serotonin returns to normal, and your depression starts to get better. We don’t understand why- but isn’t it fascinating?
There have been some reports of other types of issue arising with long term treatment, such as abnormal movements. These don’t seem to be very common and they are more controversial
DD M: Is there likely to be any permanent changes to neurobiology with long term use at all?
Andrew: Probably not – on 2 counts
We would like treatment with long term antidepressants to eliminate the need for treatment years later, by altering the neurobiology. Unfortunately I don’t think that’s what we really see. We DO see treatment effects continuing with sustained treatment over 2 years however.
We don’t see convincing changes in long term brain structure or function many many years out from treatment. There are some studies that have shown this, but its not convincing yet in my opinion.
Note from Andrew: As I look through my comments, I’m reflecting on the response I gave saying that there were no convincing long term changes in the brain with antidepressants. While that may be true, it’s more difficult to study than you’d think and there’s still work to be done there.
DD E: I am interested in things people do to ease their depressive symptoms – how much evidence is there that they help, and how much can they help relative to (or even in addition to) antidepressants? Things people might choose to do themselves without medical input like smoking marijuana or regular exercise or cutting off unhelpful relationships.
DD M: Well, there’s eating excessively or drinking alcohol too?
DD E: Maybe another way of phrasing it is “how effective can behaviour change be versus antidepressants?
Andrew: Lots of good evidence for this… CBT – people often attend to the ‘C’ – cognition/thought aspect. Changing ways of behaving was one of the core components of CBT – the ‘B’ if you like.
DD S: Based on discussions on the group, when a person first goes to their GP with depression, it seems they are likely to be prescribed antidepressants, and perhaps some short term CBT. Is that because these are the best treatments? Or are they what is most available?
Are there other treatment options?
Andrew: There are lots of treatment options, but these are some of the ones for which we have really good evidence. The advantages of antidepressants are you can start right away. There are advantages for CBT too (such as its effective, and you don’t need to take a medication at all potentially)- but you can rarely start straight away.
DD S: Thanks Andrew. Some people in discussions had felt they would have benefitted from longer term CBT, or from other talking therapies. Are those difficult to come by because they are expensive, and GPs don’t have the funding? Or is it because the HCP genuinely believes they won’t help?
What are the constraints on doctors when prescribing treatments?
DD M: Do you think IAPT is helpful as part of the treatment options?
Andrew: I think there aren’t enough clinical psychologists to meet the number of people who could want therapies and waiting lists are significant. IAPT was an NHS England initiative that helped to expand psychological treatments in England. It didn’t make it north of the border. There aren’t any constraints on doctors prescribing treatments, but someone has to be available to provide them.
Doctors usually refer to clinical psychology – who do an assessment and decide on the best talking treatment. I don’t generally refer for CBT, although I know that CBT and/or mindfulness based therapies are the more likely treatments that people will recieve. They both have solid evidence for their efficacy and lots of people find them helpful
DD S: I would say availability of providers is a constraint then:-).
Is that another advantage of CBT then? It doesn’t take a qualified clinical psychiatrist to do it, and it can be given by a nurse with some extra training.
Andrew: It can also be delivered by computer.
DD M: Do you think it is different in England, and in Wales in practice? And also for large cities e.g. London? I live in Greater London.
Andrew: I’m not sure, sorry. I think accessing psychological treatments is perhaps easier in England. I don’t know very much about Wales. I know lots of psychiatrists and psychologists in E&W and they seem to be facing similar challenges
DD N: Hi Andrew, thanks for joining us. I’d be really interested to know about the different types of antidepressants – what are the main similarities/differences and what’s the best way to find the right option?
Andrew: Different antidepressants work by affecting 2 main chemicals (serotonin and/or noradrenaline) in the brain, but in fairly subtly different ways
Some cause the brain to stop recycling them in the brain cells (e.g. SSRIs), some do this for both chemicals (tricyclic antidepressants like amitriptyline) others working in complimentary ways …. but they are more similar that they are different in a way
The *real* difference between them is in their side effects. Some medications are slightly more effective than others (e.g. amitriptyline) – but come with worse side effects. The side effects differ a lot, but their efficacy differs by less.
It’s mostly a matter of choosing your side effects initially (when I see people in clinic). For the first episode, docs generally treat with SSRIs as these are generally effective and have some of the best side effect profiles
DD T: Thanks Andrew McIntosh What is happening with these 2 main chemicals when someone has depression? You mentioned they are recycled in brain cells, can you talk about why that happens and what we know about how that changes with depression?
Andrew: The brain is designed to send signals using these chemicals from one nerve cell to another. When a message arrives at the end of one brain cell, it may be passed onto the next one using a chemical signal.
Once the chemical has done its job, the nerve cells then hover it up again, so that it can be sent again when it’s needed
Disclaimer: this is the gist, but an oversimplification
DD L: Hi Andrew, do you think antidepressants are over-prescribed?
Andrew: That’s a tricky question! I would guess that there must be some people who are receiving an antidepressant when another treatment would suit them better. However, I do not think that they are generally overprescribed.
I think the idea that antidepressants are overprescribed has been created by 2-3 things:
When SSRIs came on the market, you could achieve the recommended dose (the defined daily dose, or DDD) immediately. Whereas earlier drugs had more side effects and people often didn’t get to the usual effective dose. This led to an apparent spike in antidepressant prescriptions
The recognition of depression in GP when I was training was understood to be grossly inadequate/under-recognised. Over the last 20 years GPs have been better at spotting depression, and of course that has led to more prescriptions.
In my opinion – when someone is treated for migraine, cancer, MS etc — people rarely question whether this is appropriate or not. When antidepressants are mentioned, it’s often in the context of ‘mind altering drugs’ or ‘masking the underlying issues’. I personally believe that this is a kind of shaming/stigmatisation of people taking antidepressants that you don’t see elsewhere.
DD S: That’s really interesting. Would you say then that there was a lot of under-diagnosed depression which was sending people repeatedly to the doctors with other things? (Or, indeed, that people were just miserable a lot, without even going to the doctors…)
Andrew: There’s a lot of undiagnosed depression out there. We know that, because we’ve done studies of the general population, and we see people with depression who have never been to their GP or a psychologist or counsellor
One of the first people I treated for depression had MS. They hadn’t been given treatment I believe because sometimes people see the symptoms as understandable. I think there are a lot of people with cancer who don’t receive treatment that could help them
DD M: I was talking to a friend who worked in the pharmacy industry years ago who thought they were pushed rather forcefully by reps.
I’m guessing also that some GPs prescribed inappropriately at that point?
Andrew: I think that’s true…it’s very different now (for the better)
DD A: How do you differentiate between depression, depression from stress, depression in the context of autism, and negative symptoms of schizophrenia? Sorry, probably a weird question.
Andrew: Not weird at all. In each case, depression has to meet the same general criteria. Sometimes, it can be difficult to tell whether someone is depressed in each of these situations however as some of the features of depression overlap with that of the other condition (eg schizophrenia and lack of motivation, autism and social withdrawal). However, I think it is usually possible to tell because of the *change* in mood and behaviour in a person. It really helps to have a friend/relative there, or someone who knows the person very well.
DD A: That does make good sense, but seems not so defining. For instance, I typically have social withdrawal when depressed and lack of motivation generally. I wonder in the context of my daughters, who have been diagnosed with autistic spectrum disorder and learning disorder (learning disorder for me as well, but forgotten until I was in my thirties). In part, it is why I supported the finding a diagnosis for them, as I did not feel the treatment I received was helpful, though people meant mostly well. I will be briefly honest and say that some were not so helpful.
DD N: If money/resource/capacity were not a factor (or we lived in an ideal world with a fully funded NHS for mental health treatments) what would treatment look like? Would there be more time taken to diagnose causes of depression meaning more bespoke treatment options, for example?
Andrew: Great question! I think many issues would be the same and antidepressants would be used a lot. However, I think there would be a more rapid access route to refer people to trained therapists (e.g. nurses, other caring professionals) for straight from the GP than coming to hospital.
I’d like to think that we would also have what I’d call a learning health service.
That’s where information on your treatment is continually fed back for research and other purposes routinely so that we continue to learn what treatments work best for each individual, and we are in a cycle of continuous improvement.
DD N: yes – that makes a lot of sense! Would help the individual and the wider thoughts on best treatment practice.
DD A: massage. every. day. and trees everywhere! And government pays musicians!
DD E: Also, I have heard it said that antidepressants are like a sticking plaster over a gaping wound. It might hold you together but can never heal the underlying problems. Is that fair to say? Or part of stigmatising narrative?
Andrew: I can see that in the case of a particular individual, this narrative might make some sense. I can see people in abusive or unhappy marriages, and while they *are* helped by the antidepressant, I’m not persuaded that’s all they need to do
In some cases I think that people in very difficult circumstances can be helped to find the motivation to change their situation through antidepressant treatment.
There’s a theory of depression called learned helplessness
It’s based on human and animal research, but it states that depression happens when you no longer believe you have the agency to change your current circumstances.
You can test this model in humans and (and I’m sorry if this offends) in animals (usually rats). It turns out that there is some evidence from the animal studies that antidepressants tend to ameliorate learned helplessness
So – long answer. In summary, its complicated and its difficult to know. I don’t conclude that antidepressants are a sticking plaster however. They can be highly effective and help people help themselves out of some very intractable problems
DD A: Has there been any recent research on EMDR as a treatment for depression or anxiety?
Andrew: EMDR has been studied for Post Traumatic Stress Disorder, but has received relatively little attention as a treatment for depression as far as I know.
DD C: What is the evidence for/against the view that antidepressants might be depressogenic (causing depression) over the long term?
Andrew: I don’t think there’s any good evidence to suggest that is the case.
DD E: Having just watched the leaders debate only one, William Rennie made any reference to funding mental health. Do you have a viewpoint on mental health funding and how it could be increased. I would happily pay a bit more in tax if I was assured it went to mental health.
Andrew: I’ve just watched some of it too! I think if funding was tied to the suffering and years lived with disability in a rational way, mental health would receive more funding. I think we all need to make the case repeatedly – and write to our MP/MSPs. I wrote to Christine Jardine recently on a matter relating to mental health (she’s my local MP, this isn’t an endorsement btw!). She was surprisingly responsive and it’s worth doing if politicians think they will lose votes by not supporting mental health.
DD A: I was wondering a bit about personalized medicine. I have a sister with a CYP and serotonin transporter variant that makes her very sensitive to some SSRIs who was subsequently diagnosed with bipolar II. Do you think that guidelines to check for these types of differences will become (or should become) incorporated into guidelines? Though I know that some see it as possibly unmasking bipolar disorder, to me it seems more like feeding someone with prediabetes doughnuts.
Andrew: Interesting question – let me answer the first part
I do think that routine genetic testing will come one day. I think it is already justifiable in learning disability diagnosis and will become useful in a number of conditions soon.
I think that it will also be helpful for depression treatment targeting too. Highlighting people more likely to have a good response, as well as people likely to have side effects.
The evidence for these tests isn’t quite there yet (although there are some disreputable companies who are already offering testing)
This is an area of research we’re investigating
My hope is that genetic testing research for depression and depression treatment will be brought along and developed further as this becomes more commonplace for other conditions. I think genetics will be part of a learning health system eventually
DD A: My sister was encouraged to be tested by her psychiatrist, because of a history of developmental disorders (though not exactly descriptive, since vs IQ tends to be very high in my family, though generations, and verbal IQ catches up to normal or above). And the commentary on her genetic variations came from a phd in neuroscience (friend of mine) who said a person with these variations should never be given an SSRI. For context, they felt that my quick response to SSRI might indicate that I was a good candidate, and they had taken SSRIs in the past, so they were not anti-medication.
DD N: That’s all we’ve got time for! Thanks so much again for coming and answering so many questions Andrew.
Andrew: Thanks for inviting me along today. I hope you’re finding all of the discussions interesting and I’m looking forward to hearing more about your experience of this group some time