Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
As part of Depression Detectives, we’re holding weekly Q&As with scientists and experts who work on depression or related topics. Our Q&A last week was with Stefan Ecks, a social and medical anthropologist from Edinburgh University.
Q&A
Hi Stefan!
Stefan: Hello I’m Dr Stefan Ecks from the University of Edinburgh. I’m a social and medical anthropologist. Most of my research has been in India, on how people there experience and think about depression. I also worked in Nepal, Myanmar, and the UK.
Much of my research is also about how psychotropics are used, esp. Antidepressants.
Depression Detectives member S (DD S):So what differed between how people in the U.K. experience and think about depression, to how people in India do?
Stefan: There are so many differences! When I started studying this in the late 2000s, the word “depression” was still quite uncommon in India. People would use a whole range of other expressions, which had some overlaps with English “depression” but never matched.
Then the medical treatment is different. There is almost no counselling or psychotherapy.
DD N: Do you think that means they were experiencing something different, or talking about the same thing in a different way?
Stefan: Both: different experience, different expression.
DD J: I was wondering something about demographics of areas and how that works with what seems to be a lot of services provided by charities. Is there any indication that this shuts out or misses some groups of people? Are there geographical areas/demographic groups that seem to have more options available than others due to what charities are operating where?
Stefan: In the UK, the vast bulk of treatments is given by NHS GPs. This is, as far as I know, fairly uniform across different areas of the UK, though you have some regional variations in just how many people are given drugs. I would also guess that deprived areas have much higher rates of people getting treated with drugs than richer areas. Charities focus on non-drug counselling.
DD S: Stefan, you said ‘when you started studying depression in India’, have you found it’s changed over time? And would I be right to guess that different demographics have changed first?
Stefan: A lot has changed, treatments for depression have become more common and most people now also understand the term “depression”. I worked a lot with Indian pharmaceutical companies that produce antidepressants, and it’s clear that their products are now used across the country, even in remote rural areas.
I was also surprised that antidepressants are prescribed by so-called “quack” doctors, which are very common in rural areas. They are using antidepressants routinely now.
Changing demographics are also at play, but most important is more awareness and less stigma
DD N: Are quack doctors unqualified people acting as doctors?
Stefan: Yes, they have no license and are technically illegal, but the police tolerates them because there aren’t enough licensed doctors.
DD S: I guess I was wondering if more affluent, possibly more westernised, Indians changed their ideas about depression first?
Stefan: Yes, that’s the case. Though epidemiological studies show that people with lower education, income, and socioeconomic status are more prone to depression.
DD S: But are they all equally ‘allowed’ to have depression? I mean, I’m thinking of my grandparents generation, where, you know, it was ok to go to the doctors with a broken arm, but mental health challenges, you were just expected to get on with.
Stefan: 20-30 years earlier people would have interpreted the symptoms differently. E.g. there was a very strong spiritual mode of interpreting depressive symptoms, and the recommendation would have been to seek a spiritual cure, e.g. praying, going to temples, meditation, speaking to gurus.
Depression as such has never been much stigmatized, whereas many other mental disorders were, esp. Schizophrenia.
That idea of “just snap out of it” has definitely been very strong in India as well. Just get on with it: it’s something that even a lot of Indian GPs would have told their patients.
DD S: That’s really interesting. I’m wondering what advice a priest would give someone who went to them for their depression, and whether it helped.
I’m also wondering if in the past, people in western countries might also have gone to see the priest or vicar about their melancholy. And whether that helped?
DD I: Organised religion can be both a help and a hindrance (e.g. for many it provides additional community support and people to turn to for help. But sometimes mental health is regarded as a punishment for sin / consequence of not praying hard enough or doing the right rituals.
It would be interesting to hear if Stefan has noticed any difference between countries / religions.
Stefan: Fascinating question. Christian religion is quite well known for making people anxious about “sin” and its consequences. But it’s not linked to “depression.”
Stefan: In India I heard countless time how everything is “in God’s hand”. I think this really helps people to cope with adverse life events. Bad things don’t get internalized, and there’s no need to feel guilty about them. It’s fate.
DD S: An aid worker in Nepal told me that in his experience Hindus were sometimes sceptical, or downright antagonistic to aid work. Because they thought poor people were poor because of how they’d behaved in a previous life, and there was no point trying to change it…
DD C: Such an interesting question. Related to that, I wonder if negative effects of religion on mental health might be connected with something called “spiritual bypassing” – ignoring emotional and personal issues for the sake of the spiritual. For example, if people feel that they need to forgive others before they have stayed with and worked through feelings of pain or anger. Would you say this happens in Indian religions, too, Stefan?
DD C: Could you tell us a bit about whether social and economic changes in the West might have contributed to a rise in depression?
Stefan: This is one of the most important questions! because depression is such a paradoxical problem. With almost any other disorder, the richer people are and the more treatment they get, they either don’t get it or they get better. Depression keeps rising at the same time as antidepressant prescriptions are skyrocketing. The drugs should reduce the number of people with depression, but there is no sign that they do. And why is it rising so much? this is something that the Indian doctors are also very concerned about: they think that life in the past was better compared to now, less stressful.
DD N: Do you think that the rise in depression is due to more people who had depression anyway being diagnosed? Or do more people have depression now?
Stefan: The trickiest question! We’ll never have a clear answer to it because the awareness of the diagnosis (and the drugs) change the experience, and change the number of people suffering from it. All we know for sure is that, even in India, more and more people are reporting with symptoms of depression, as well as more and more getting treated.
There is a lot in India’s pluralistic medical system (with a strong presence of Ayurveda, homeopathy, etc.) that offers alternative diagnoses, and alternative treatments.
DD N: Does the difference in culture around family / social support make a difference in other countries? We have quite an individualistic culture in the UK.
Stefan: This is a key assumption, and I think it’s true. There was a fascinating set of studies done by the WHO in the 1960s on recovery from schizophrenia, and India came out as far better than the UK, and the explanation was that family/community support is so much stronger there.
This question of “individualism” has many further aspects. One of them is that Indians used to live in large joint families, including 3-4 generations. There was much less “individualism” when you live with 15-20 other people.
Also, depression has to do with a disordered sense of “value”. I think depression is rising with rising individualism is that one’s selfworth is never secure. There is a deep connection between modern forms of capitalism and depression in this regard.
DD N: It’s a big question but… do you think there’s any way of fostering that kind of community support system in places that don’t have it?
Stefan: I think community protects against depression. If community can be fostered from the outside, rather than be built by people themselves, I’m not sure.
DD C: Could you explain a bit more how capitalism and depression are related? And what a disordered sense of “value” means?
Stefan: In its current form, capitalism asks people to constantly be better, to improve, to strive, etc. That easily creates a feeling of “never enough”. No matter how much work you do, no matter how much money or esteem you gather, it will not be “enough”. That’s one reason why capitalism creates a kind of “rat race” feeling of stress that people arguably didn’t have. Also now people work in service industries, and being creative and “self-driven” is so much more important for many jobs. Any shortfall in “creativity” or “drive” or “enthusiasm” will be so much more noticeable. I imagine that, 100 years ago, farmers didn’t need quite as much self-driven enthusiastic creativity for their work.
DD S: Thinking about *within* a country, do different demographics or cultural groups experience depression differently? Do some groups get it more or less? Do different groups react to it differently? Seek different sort of treatment?
Stefan: It’s generally agreed that low income, low education, and living in relatively deprived areas (esp. if affluent areas are close by) make people more prone to depression.
DD I: So it’s more about relative poverty compared to your neighbours than absolute levels of poverty (e.g. income compared to another country).
Stefan: Yes, it’s relative status. This is the most important factor, I think, and way too little research is being done on this. Because how much money someone earns is so much easier to study than how this amount of money “feels like” compared to others around oneself.
Richer people tend to be more suspicious of drugs, and tend to seek nonpharmacological therapies more.
DD S: Or is it just that richer people can afford to pay for more non-drug therapies?
Stefan: That too. It’s a big problem that non-pharma therapies are often far more expensive. E.g. there is a lot of non-pharma psychotherapy also in South American countries, but it’s entirely the preserve of the richer people.
DD S: But, eg, the stereotype would be that men find it difficult to talk about their feelings. And might be less likely to admit they aren’t coping, and seek treatment. (And are more likely to die by suicide).
Older generations might set more store by being ‘stoic’, and there is maybe a perception that younger people are more open about mental health.
Stefan: Gender differences still play a big role, yes. I think a lot has changed in the UK here though.
DD N: That’s all we’ve got time for! Thanks so much for coming Stefan, this has been super interesting.
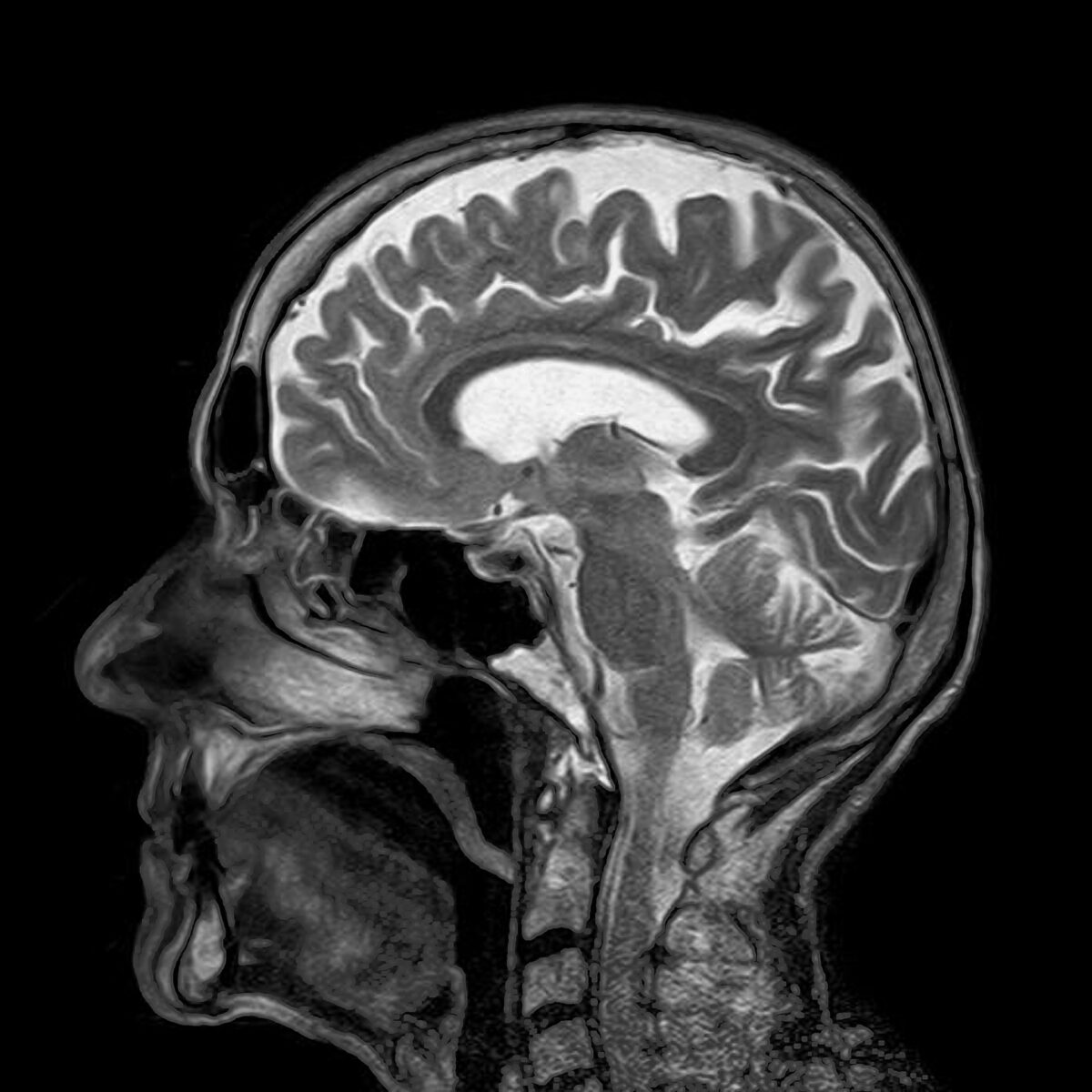
Depression Detectives is holding weekly Q&As, which are a chance for us to to quiz scientists and experts who work on depression or related topics. Last week we were joined by four scientists from Edinburgh University – brain imaging expert Heather Whalley and her colleagues Niamh MacSweeney, Miruna Barbu and Liana Romaniuk.
Q&A
Hi all!
Niamh: Hello everyone! My name is Niamh and I’m a 3rd year PhD student at the University of Edinburgh. My research looks at the biological, psychological and social risk and resilience factors associated with adolescent depression. I am particularly interested in how our brain structure and function is related to depression risk, and other social/environmental factors.
Heather: Hello – I am Heather. I am a Reader in Neuroimaging in Psychiatry at the University of Edinburgh. My research involves examining brain scans to look at depression, and looking at associations with various risk factors
Liana Romaniuk is here also – she is a child and adolescent psychiatrist with a background in brain imaging and can answer any clinical related questions
Miruna: Hi everyone! I am Miruna. I am a research fellow in the Division of Psychiatry at the University of Edinburgh. I study depression and its genetic risk factors, as well as how these relate to environmental variables. I also study something called DNA methylation , which is a process through which our genes can be “turned off or on”. I am trying to identify whether these patterns are different in depressed individuals as opposed to healthy individuals.
Depression Detectives Member C (DD C): Can you tell us in what way a depressed brain is wired differently to a non-depressed one please?
Heather: Good question! There has been a lot of research over several decades to try and work that out and we are only now beginning to understand. More recently there has been an effort to increase the size of imaging studies (10s of thousands of individuals) and they are highlighting some interesting and convergent findings. We are seeing decreased hippocampal volume (a region involved in emotion and memory), decreases in the cortex of the brain, particularly in regions considered to be involved in thinking/planning/reasoning. Decreased ‘healthiness’ of the brain’s connections (white matter), and altered functioning when the brain is at rest, and when it is performing certain functions. The disruption of connections, structure and function of the regions considered to be involved in emotion and reasoning are thought to underlie the core features of depression, low mood, low motivation etc.
DD C: Thank you. Have there been any studies looking at how this changes over time in individuals? It would be so interesting if there were a prospective cohort study in which well people were scanned at baseline the followed up over years and rescanned if they developed symptoms of depression to see how their brain had changed or if there were predisposing factors present.
Heather: yes – this is spot on! We are currently looking at a very large study based in the states that has scanned >10,000 9-10 year olds where they hope to follow them up over 10 years, and although their study isn’t specifically focused on depression – we in Edinburgh are hoping to study this exact point you have made.
DD C: So good to hear that you can study this on such a large scale.
Heather: also we and others have conducted very similar studies in the past (although in the 100s, not 1000s!) for those at high risk of schizophrenia and bipolar disorder who were well when recruited, and we then followed them with repeat scanning over 10 years.
DD C: That sounds interesting. Is the picture for people with bipolar disorder similar to those with depression? I do wonder about whether the depression experienced by people who only go low is the same entity as in those who swing between high and low.
Heather: actually in the study we conducted above that I mentioned, the majority of the young people that developed an illness in the bipolar high risk sample actually developed depression in the first instance. In this case it is difficult to know whether this is just the typical manifestation of bipolar in such a young group – or whether they would go on to just have low mood. We are actually following these people up using healthcare record linkage to try and tease this apart. Note: ‘high risk’ here refers to familial risk factors, and study participants were not told they were in the high risk group.
DD C: It would be interesting to know whether being told you are high risk for bipolar or depression makes it a self-fulfilling prophecy!
Heather: Ah – i could have worded that better – familial risk and of course we were v sensitive
DD C: I am sure you didn’t do anything to harm your study participants! I was thinking more about it in the real world, rather than the lab setting.
DD I: This feeds into the current diagnostic arguments about bipolar illness, particularly the concept of the BP spectrum. With regard to depression/bipolar, many are diagnosed with depression as the presenting symptom but are later diagnosed with bipolar. Depression by its nature is often the more distressing feature of bipolar illness. GPs who are the first port of call are poorly equipped/resourced to differentiate the subtleties of bipolar illness and therefore wind up treating the depression. If as some believe this can exacerbate bipolarity, it reinforces the need for better diagnostic criteria and skills in general practice. This in turn exposes the relative poverty of available treatment (especially in children and young people) both drug and psychotherapy. We could then venture into the minefield of over/under diagnosis/treatment of mental illness. It all underlines the desperate need for better diagnosis and treatment/therapy. Bring on the day when mental illness is diagnosed by a blood test.
Heather: Yes absolutely! It also speaks to the difficulty in diagnosing young people at early stages of illness, not just depression and bipolar disorder.
DD S: Can you tell us a bit about what brain imaging can tell us about what happens in depression?
Niamh: Brain imaging is a relatively new technology, which means that it has really allowed us to expand our knowledge of how the brain works and differences that may occur in mental health conditions like depression. At the moment, brain imaging research looks at patterns in brain structure and function, such as brain volume as well as white matter tracts, which connect different brain regions, to see if we can identify whether there are differences in people with and without depressive symptoms. We need really large samples (thousands of people) to answer these research questions but thankfully in recent years, there have been lots of large-scale brain imaging studies that have greatly developed our understanding of depression.
DD S: What kind of things can you actually see with brain imaging? Are you seeing that some brain structures grow or shrink? Or are you seeing which bits are active or inactive?
Niamh: Good Q! It’s a bit of both actually depending on what your research question is. In terms of brain structures “growing or shrinking”, we can only see this if we use multiple data points over a period of time, which is known as longitudinal data. Further, we are looking at brain changes at what is called a group level – so on average across a large sample of people. With the development of large scale studies, it will be really exciting to look at how brain features change over time, especially in adolescence, when there is so much happening in the brain anyway. In terms of brain function, we do a special kind of brain scan, called a functional MRI (fMRI)- this allows us to look at what parts of the brain are “active” when a person is performing a certain task or just at rest. For example, we are currently running an fMRI brain study where we are looking at what parts of the brain are active when a young person with depression is irritated. To study this, young people are asked to read irritating scenarios in the scanner and imagine they are in that situation. We are then going to use data analysis methods to see what parts of the brain are active.
DD S: You said the ideal would be a longitudinal study. Can you use brain scans done for another reason as your baseline, to compare across time? To get ‘before and after’ pics? eg if someone has had an MRI for another medical reason, and then later gets depressed.
Niamh: This is a super Q and very relevant to large scale health research at the moment. There’s a lot of debate currently on whether researchers should have access to routinely gathered medical records to get a better overall picture of someone’s health, and then also to use any pre-existing health data (e.g., an MRI scan). This question is particularly pertinent because often the people that take part in research studies are not representative of the population at large. Research participants are more likely to be women and from higher socio-economic and education backgrounds. If we had access to health records, we may be able to include people who don’t have the time/opportunity to take part in research, and this would hopefully give us a better picture of whatever we are trying to study. However, lots of the population-based studies do try to combat this bias by recruiting as diverse a sample as possible but this can often be difficult.
DD C: Somebody in this group earlier asked if a depressed person’s brain changes with treatment (whether that be medication, exercise or talking therapy)? And can depression really, physically be ‘cured’?
In regards to the size of the hippocampus in depressed people. Does this show signs of improvement with treatment? Or are these people’s hippocampus already smaller? Predisposing them to depression?”
Very nice to be here – and again a great question. What we don’t really know as a field as yet is whether the brain changes that we see in depression are a cause of the illness, or actually a consequence of having the illness or medication. This is because most large studies are conducted in adults in mid-late life, and they tend to only capture a snap-shot of an individual. What we need to understand these features is what is called longitudinal data (collecting data from an individual at several time points over illness and treatment). Also, what we are interested in is imaging young people before they become ill in order to address the question as to whether the brain differences happen before illness onset, or after. This is important to know if we are thinking of being able to predict those who are vulnerable to illness, or to understanding pathways to illness, what happens during illness, and for developing novel treatments – or to targeting treatments to an individual.
DD I: In the previous Q&A there was a discussion about the difference between adult and adolescent depression. Can that difference be seen in brain imaging or methylation?
Liana: Absolutely: there’s definitely a lot of overlap in the symptoms adults and adolescents with depression experience. There’s some evidence to show that adolescents are more sensitive to being rejected by their peers, and tend to be more irritable – above and beyond what plays a normal part of adolescence. In terms of treatment, similar medications are used for both age group, although we’re especially safety-conscious with younger people, and so use a smaller range of tried-and-tested medications. The psychological treatments are crucial, and carefully adapted depending on the age of people we work with.
Heather: as a follow on – we are currently conducting a study to look at irritability in adolescent depression – during a functional imaging scan.
DD I: What is the difference between a ‘functional’ imaging scan and a normal one?
Heather: There are different types of brain imaging – we focus on Magnetic Resonance Imaging (though there are others for example that are used clinically like CT, or for other types of research like PET) – a functional MRI scan like I mentioned above allows us to look at which regions of the brain are ‘activated’ by a task or question. (this is actually due to a really cool quirk of nature related to the fact that oxygenated and deoxygenate blood have different magnetic properties). Other types of scan allow us to look at things like brain volumes of different regions (structural scan) -or allow us to look at the brain wiring (white matter – called diffusion imaging).
Niamh: Really interesting Q. We’ve recently done some work looking at whether the differences in brain structure we see in adults with depression are the same or different in adolescents with depression. We do indeed see similarities between adult and adolescent samples. For example, compared to people without depression, both adolescents and adults show a decrease in brain volume as well as impairments in white matter tracts/connections, especially in areas relating to emotion/thinking processes. However, we do see some differences too — adolescent depression was associated with lower brain surface area, a finding that we don’t see as commonly in adults with depression. This suggest that these changes in brain structure may be present early in the disease course of depression, and may be linked to the emergence of the disorder. However, as Heather mentioned, we only looked at a “snapshot” of depression and brain structure in these young people, i.e., we only had access to data at one timepoint. We really need to look at brain imaging data over multiple years, especially before the onset of symptoms, to really understand how brain features relate to depression, and what features are a cause or consequence.
Liana: This is really exciting because it’s quite novel within the field.
Miruna: In terms of DNA methylation, this field is very novel, especially in terms of associations with depression. In our department, we are trying to identify DNA methylation differences in adults, and we have identified some differential patterns that could add to our understanding of depression. Studies of adolescents have definitely shown DNA methylation differences, although large-scale studies are needed to determine if these are similar to those differences in adults. DNA methylation is also something that changes a lot throughout life as a result of environmental factors, so patterns in adolescence may not necessarily be the same as patterns in adulthood.
DD I: So things that we experience/do can alter our DNA methylation pattern?
Miruna: Yes, that’s right. For example, smoking greatly alters DNA methylation patterns. Smoking is also known to be associated with depression (smoking may increase your risk of being depressed) – so it is possible that one route through which smoking increases this risk is through changes in DNA methylation patterns. This is just an example, but DNA methylation plays a big role in other lifestyle factors as well, such as alcohol consumption and body mass index.
DD I: And if someone stops smoking?
Miruna: This is quite interesting – studies show that peoples’ DNA methylation patterns go back to looking like those of non-smokers, although this happens over years. In relation to depression – we have yet to understand whether depression risk is lowered as a result of this change (although quitting smoking is sometime tied to starting healthier activities, such as exercise, which increase well-being and are protective factors against depression).
DD N: Do you know if you can look at what’s happening in the brain and see a difference in activity in the same person when they’re depressed and when they aren’t, as opposed to changes in the structure of the brain?
Niamh: At the moment, we are quite far away from being able to detect changes related to depression on an individual level — i.e., having a brain scan to diagnose depression. This is because there are so many other factors related to depression risk, such as genetics and environment. Also, the development of large scale brain imaging studies will allow us to map out what “typical” brain development looks like across the lifespan — kind of like creating a growth chart brain development. Only then will we be able to identify divergences away from “typical” development, e.g., towards mental ill-health. However, it is very unlikely that we will just be using one factor to determine risk and resilience for depression — using a combination of factors will give us a much better picture.
DD S: Can I ask a basic sort of question, what techniques do you use? What exactly are you looking at?
Liana: One of the major techniques we use is magnetic resonance imaging – MRI – which is a fantastic way of taking detailed 3D images of structures like the brain, and has the added bonus of using no radiation, although it is pretty noisy! Its an amazing application of physics, where strong magnetic fields are used to align all the water molecules in our body, then other quickly-changing magnetic fields gently “flip” those molecules, and when they relax back to the centre, they emit a radio signal that we can detect. Different body tissues emit different signals, so we can reconstruct all these to generate 3D images. And if we do that quickly, and key in on signals associated with shifting oxygen levels, we can see the effects of changing brain activity over time.
Our top-notch scanners can take a detailed picture of your entire brain every 1.5 seconds at the moment
DD S: Wow!
DD J: If there are differences in a depressed person’s brain, could there be a screening programme for depression, like there is for cancer?
Miruna: Really good question! At this moment in research, I believe we are quite a long way from having a “brain-based” screening test for depression. This is because what we are observing in our studies are associations between specific changes in the brain and depressed individuals. Association alone will not tell us whether a person will definitely be depressed or not based simply on brain morphology. Moreover, apart from differences in brain, there are a number of other factors that may signpost whether an individual will actually become depressed (for instance, environmental or genetic factors). However, there is work going on at the moment to identify whether the function of these brain areas are different in depressed vs healthy individuals, and I think this field is making great strides, especially in adolescent research. I think in future, once we identify more definite risk factors for depression, we may be able to have a screening test for depression and be able to identify signs early on.
DD S: When you say ‘association alone’, is it possible that some people have those brain features and aren’t depressed, and other people are depressed without having those brain features?
Miruna: Hello! Yes, it is – as you say, some individuals may have brain features that resemble those of depressed individuals and vice versa. However, in our studies, we apply statistically-robust tests, so we can say with confidence that at a general population level, our associations are “true”. When it comes to an individual screening test, individual differences such as the one you mentioned may lead to someone being classed as depressed when they may not be. This is why studies often talk about replication, which refers to independent groups of researchers obtaining the same result multiple times – to make sure the difference is really there!
DD C: Is there any relationship between the areas of the brain affected in depression and those involved in memory? I find I struggle to remember things from the times when I was having a serious bout of depression, as opposed to everyday background levels when I was able to keep functioning.
Heather: yes, the hippocampus – one of the most commonly reported regions identified by many many studies, is thought to be involved in emotion and memory particularly. Though the thoughts at present are the depression isn’t likely to be due to a problem in one brain region in isolation, but a network of regions not interacting as they should. Emotion and memory of course are also v strongly linked. Events that illicit an emotion will usually be more strongly ‘encoded’ and remembered.
DD C: so if you are struggling to feel any emotion, for example in dissociative depression, then you may not create such strong memories?
Heather: Yes- well put! Though it is difficult to know which direction this might work in, in depression.
Liana: Just to add to that, we also know that memory encoding is very dependent on having relatively steady attention and concentration (which are processes drawing from broad brain networks). Sadly having disturbed concentration is one of depression’s more debilitating features, and that definitely goes hand in hand with the sense of not being able to remember things.
DD I: Sleep is also important for memory? And affected in depression?
DD C: ah yes, I forgot that 😂Excellent point. Is there a reason behind the disturbed concentration?
Liana: Ah, sweet irony! Concentration is a process that really does engage large portions of the brain’s cortex, as well as the deeper structures that coordinate activity around the brain – several structures and neurotransmitters play an important role, and its probably why concentration can be affected by many illness.
Sleep is also really important for “consolidating” memories – taking those experiences of the day, which are represented in a temporary way, and converting them into more robust memories by changing the structure of brain synapses.
DD C: Would you say that changes in volume in the different areas could be caused by the way people think? Asked the other way around: Can therapy potentially change the brain in a positive way?
Heather: I think that we just don’t know the answer here, there just aren’t enough large scale good studies to say for sure. There is a literature that has looked at differences in the brain between people experiencing a current depressive episode versus those that have recovered – or don’t currently have symptoms – but it is still unclear. Studies aren’t converging in a convincing way (I would say) – others may like to chip in here
DD I: Do different types of depression lead to different changes in the brain?
Niamh: We don’t yet know really but this is definitely a hot topic in depression research! Depression can present itself in many different ways and is often referred to as a “heterogenous” condition. We should be able to answer your question soon as more large-scale studies become available 😃
DD N: That’s all we’ve got time for! Thanks so much for coming Niamh, Heather, Miruna and Liana.
Liana: It’s been a really pleasure – the questions were all excellent and insightful!
Miruna: It was a really great experience! Thank you so much for having us – the questions were great!
Niamh: Thanks everyone for the great questions! Really interesting discussion 😃
Heather: I hope that has covered most of the questions – happy to answer anything outstanding offline. That was great fun – thanks to everyone for organising /asking qu and answering! Its really invaluable as researchers to think about all these questions (and new ones) in a different way. Thanks for having us!
DD C: Thank you all – such an interesting experience although it just makes me come up with more and more questions……
Depression Detectives is up and running, and we’ve kicked off our weekly online Q&As! These are a chance for the group members, with lived experience of depression, to quiz scientists and experts who work on depression or related topics. This week we were joined by clinical psychologist and researcher Stella Chan, and this is the transcript of that conversation. We’ve removed names and any identifying information to keep the contributions anonymous.
Q&A
Hi Stella!
Stella: Hi all, I am a clinical psychologist based at the University of Reading. I have been doing research on depression for some years. My current focus is on adolescent depression. Hello to you all.
Depression Detectives member A (DD A):
Thanks for taking the time to be here today. I’m a bit confused about (apparently) conflicting views on depression and medication. Some GPs have said that one should try and “come off” antidepressants after CBT practice etc. is well established some have said there’s no rush and no long term issues with medication, so don’t rock the boat. Is depression seen as a temporary illness which you can “think” your way out of, or a chemical imbalance (that might be inherited), which taking long term medication for (like diabetics take insulin) is expected. I’m simplifying the views I’ve heard but hope you can give us your opinion.
Stella: It’s difficult to say. There have been mixed research findings. The common view is that depression is caused by multiple factors – biology (e.g. genetics, brain functions etc), psychology (thinking and feeling) and social (environmental and relationships etc). But of course the cause for each individual is different. Regardless of what causes depression, one finding that is quite established is that depression itself tends to be ‘episodic’ – meaning that it’s like a TV episode, it comes and goes. Some people experience one-off episode but some experience recurrent episodes over time.
Advice on treatment also seem to vary across different professionals. My own advice is that there are a lot of individual differences – the advantage of CBT (and other psychological treatments) is that individuals are given help to learn more about themselves – to develop their own coping strategies, versus medication is more passive. So, psychological treatments give people a better chance to prevent the next episode if they feel able to implement the coping strategies. That said, I know people who really benefit from ‘maintenance medication’ i.e. continue taking medication after you have recovered for a little while to consolidate recovery.
People really vary so the best is to work closely with the clinicians who look after you to determine the best strategy – but also be prepared to ask questions and don’t feel you have to accept whatever treatments offered to you.
DD I: Are there different types of depression?
Stella: This is a big research question actually. Research on depression has generally been rather slow, with little breakthrough in the field compared with other conditions like anxiety. Some researchers have proposed that depression may have different subtypes which we have not identified yet – and that’s why treatments don’t always work because treatment offering isn’t tailored to subtypes. One example is that some people experience ahedonia (i.e. lose pleasure of things they usually enjoy) but some don’t (instead they feel sad). It’s common to lose sleep in depression and yet some experience the opposite (sleep too much).
DD N: I’m curious whether this may link in some way to some depression being a result of other mental health issues or neurodivergences that haven’t been properly diagnosed or treated? Because living with these other issues has caused a situational depression therefore there’s a variance in how it presents to depression that is mainly biological?
DD N: I have also done some reading around physical causes of depression, has much research been done into this? From a female point of view, the impact of monthly hormonal changes and how this can impact mood? It seems like this regularly gets dismissed by GPs, but can have a massive impact on daily life when you have 1 week a month when you experience symptoms of severe depression
Stella: Yes I totally agree. there are many layers here actually – depressive experiences/ symptoms could be different when people have other mental health difficulties or neurodiversity. This may lead to clinicians having overlooked / missed some of them. We are developing a new screening tool for depression for children and young people with autism for exactly this reason. I also think that sometimes clinicians may not be paying enough attention to signs of depression when there are other mental health problems present that have ‘distracted’ their attention. Same for family and friends and other professionals such as teachers and support services. Not saying people are careless or anything like that, but real life clinical work is not like textbook and things are often unclear.
DD N: Thanks Stella, that makes sense – it’s such a complex issue because we all have very different experiences. Do you think in some respects ‘textbook’ definitions of depression can be a hindrance in diagnosis and treatment because they frame it in isolation from other issues?
Stella: My short answer to that question is that yes – i think textbook definition may need to be revised following research. It is also important to understand that depression is not a label but a subjective experience. The bottomline is that if you are experiencing a hard time, feeling low and depressed, you don’t (and shouldn’t) need to tick all the boxes to justify that you need help. If you feel you are not coping then help should be offered. It is also important to balance between theoretical/ medical perspectives and practical everyday aspects. Sometimes the solution involves more than changing the way you think and feel, but it may be about some practical changes in environment. I have once helped a young person who was referred to me for depression but after a few sessions I think what they needed was some time off having some fun (as the young person was a carer for a family member). In the end instead of psychotherapy I referred them to young carer charity’s support and it did a whole lot of good.
DD S: Depression pertaining to psychology is a persistent low mood that affects a persons a persons behaviour, their thoughts, feelings, motivation and their sense of wellbeing and is marked by such features as sadness, low self-worth, lack of concentration and clear thinking and an inability to enjoy life. During a person’s experiences of depression a person may encounter the following symptoms: The feelings of deep sadness, dejection, hopelessness, a pessimistic outlook, low self esteem, an increase or decrease in appetite, altered sleeping patterns, a reduction in energy levels, altered reaction times, a decrease in the ability to take pleasure in the ordinary things of life and suicidal tendencies.
Stella: Yes – though it’s important to stress that you don’t need all the symptoms to be diagnosed. This means that individuals who have depression could have different symptom patterns, which may suggest different subtypes but research hasn’t been very clear yet on this point.
This is true of most of mental health illnesses, there is a lot of research but the causes are hard to define or know what are the root causes. Each person is different and as you have already mentioned it could be due to a number of different causes which contributes to a person’s symptoms.
Also because most research is cross sectional (i.e. one time point) – and these results can only tell us what factors are ‘associated’ with each other but can’t tell us which causes which. For example, people with depression often have sleep problems, but it’s difficult to say whether sleep deprivation causes depression (it’s possible as we all know how crap we feel when we haven’t slept well) or whether depression keeps people awake (which is equally possible as we all have nights that we lie in bed ruminating about our troubles). Longitudinal studies (i.e. studies that have multiple time points) are difficult to conduct – people often drop out (i.e. participants stop taking part) and it’s expensive to run.
DD S: There are different things that we know predispose someone to depression – e.g. certain genes, adverse childhood experiences, etc. But why can two people have the same predisposing factors, but one person develops depression and another one doesn’t?
Stella: Yes that’s a very important question. I think one reasonable explanation is the stress diathesis model, which suggests that people have background vulnerability and when the background risk is triggered by stress then one may become unwell. So, level of stress, as well as the level of stress coping skills, and reactivity to stress, could make a fair bit of difference
Similarly, social support and relationship quality will also make a difference. In short, we all have risk and resilience factors and our chance of getting depression and our ability to bounce back/ recover is perhaps a balance between the two.
DD S: Are there things a person can do to improve their stress coping skills, and ward off future episodes of depression?
Stella: Yes, absolutely. Shirley Reynolds has published a few nice books on teenage depression (for young people and for parents I think). In general, I would suggest going back to basics: sleep well, eat well, regular exercise, connection with nature. These are all evidence based actually – though also sounds common sense. In terms of cognitive skills – I think avoid black and white thinking or jumping into conclusions; instead try to put things in perspective and ask yourself what would you say to your best friend if they have experienced this situation. I would also highly recommend having a look at self-compassion self help – self-compassion is different from self esteem; it is about showing kindness to yourself at times of disappointment and setbacks. It is closely associated with depression.
I would also recommend behavioural activation – this does not mean you keep yourself insanely busy, but to make sure that you engage in activities that you see value in them.
I think relationships and social support are really important. It doesn’t have to be romantic relationships at all – friendships, family, or even people you see in hobby groups.
DD S: Hi Stella what’s your view on “Lifestyle Management Courses” Like the one run by [removed for anonymity]?
Stella: I can’t comment on this particular course because I don’t know much about it. That said, the key is to see if the course is ‘evidence based’ (i.e. whether what is offered has been tested and evaluated to be effective).
DD S: I am a peer volunteer for a Lifestyle Management Course and facilitate on the course. the success rate of the course can be seen in the looks of fear and trepidation that are on the participants faces when they walk in on week one to the smiles they leave with at the end of week 10. LMC has four main components: 1. Relaxation/meditation 2. Weekly self-management education topic 3. Weekly solution focussed reflection 4. Gentle graded Movement.
A 10 week 3 hours per week course co facilitated by Practitioners and Peers.
DD S: Is it true that some people remain stuck in the cycle of depression because they have adopted poor habits of allowing those habits to control them and thinking that nothing can be done to help them out of the situation?
Stella: It’s rather difficult actually – when people are depressed, one of the classic symptoms is that they feel hopeless and they lose motivation. These symptoms make it very difficult for people to engage in therapy to change the way they think/ cope.
I also want to emphasise that it’s not all about individuals. Our environment is key as well – being placed in a supportive environment, good access to treatment and support, with supportive relationships etc go a long way in empowering people to develop new coping skills. Life is hard though and sometimes the lack of control is not purely psychological – things are often out of control. More integration between social support and individual therapy is important, in my opinion. We need to recognise the importance of the interaction between environment and ourselves
Also echoing one of the comments above about the possibility of subtypes of depression – it’s possible that some depression is more ‘chronic’ by nature due to its causes. We don’t have enough research findings to know whether this is exactly true, but I do think that from clinical observation, people with depression vary a great deal.
DD I: You mentioned adolescent depression in your intro. Can you say something more about that? Is it different from what adults experience or a precursor to it (or some other interaction?)
Stella: if you look at a diagnostic manual, the only one difference in terms of symptoms is that ‘irritability’ is listed as a symptom in children and young people but not in adults. Personally I am not sure if I am convinced that this is a key difference. I think irritability is a symptom across age groups (not for everyone of course).
Current treatments for children and young people with depression tend to be adapted from adults – and they are not very effective (their outcomes are poorer than that in adults). I think we need to develop better treatments that are based on our understanding of young people’s everyday experience and if possible involve young people using a co-production model. We are actually running a series of three workshops over the next half year to discuss adolescent depression.
DD A: The stereotypical portrayal of an adolescent is of someone going through rapid hormonally-influenced changes and so their behaviour is irrational, selfish, unpredictable etc. What do you think about these stereotypes and can they mask more serious mental health issues that adolescents might be experiencing?
Stella: yes I agree these stereotypes are rather unhelpful. We take time to grow up – and scientifically speaking, our brain is developing until around age 25 (yes!). Sometimes young people may seem to be inconsiderate but I do wonder if this is something to do with their high level cognitive functioning (e.g. perspective taking etc) being still developing. I think the stereotypical portrayal of ‘moodiness’ is indeed a key concern that masks mental health problems. Another concern, a serious one in fact, is that some young people with depression are misperceived as attention seeking or drama queen that sort of things – one of my MSc students have analysed lots of social media posts which reveal that this is indeed a widespread issue. These add to more stress and sometimes makes young people hesitate to seek help.
DD S: Hello, CAMHS psychologist here, you’ve talked a wee bit about secondary depression to other presentations such as anxiety or neurodevelopmental conditions. What are your thoughts on the order of treatment? You also mentioned about how the treatment options for young people are adapted for adult treatments and less effective. Are there any up and coming therapies that are looking promising?
Stella: In terms of order of treatment – i think it depends on individual cases. Once I had a case that was depression coupled with alcoholic use – the issue was that it was difficult to engage the service user in depression treatment when they were not sober. Hence the decision was made to help with alcohol use first. One way to decide is to open up the question to the service user and ask whether they feel one is driving the other or whether they feel if they feel more confident that one is more modifiable.
In terms of treatment – i think behavioural activation has shown quite good results with young people (because cognitive work is more effortful and difficult for young people).
DD J: I was wondering if your research includes ADHD? I’ve found personally, that the symptoms and results of ADHD greatly increased depression. I wish my doctors looked into ADHD first instead of just treating my depression and leaving an underlying factor unaddressed.
Stella: I have collaborated on work on ADHD (led by Sinead Rhodes) but it’s not something I have specific expertise in. I definitely think our understanding of depression in people with ADHD, Autism and other developmental conditions is not very good because most of the research has been on people without these conditions. I would encourage you to challenge clinicians’ views if necessary if you think they have overlooked anything.
DD N: If you’ve got time at the end Stella, it would be great to know if there’s anywhere you think there are gaps in depression research that should be looked at?
Stella: Too many gaps in research – I would prioritise involving the voice of young people in research. We have just launched a survey to ask young people what they think we are missing in research in depression. My own motto always is ‘ask the people you want to help’.
That’s all the questions we’ve got time for unfortunately! Stella thanks so much for coming, this has been extremely interesting to read.
Stella: Hope people have got something out of the hour. Take care – my goodnight message is to take it easy – life is hard, and we don’t have full control over what happens in our lives, nor can we always control how we react in situations. We feel as we do as humans. Take it easy, and be kind to yourself as you would to someone you love. Goodnight x
Depression Detectives was a user-led citizen science project that ran between March and September 2021. It brought together people with lived experience of depression, and researchers who study it, as EQUAL partners. The aim was to get researchers listening to and working with non-scientists and put lived experience at the heart of research.
Volunteers took part in online conversations with researchers studying depression, to find out what science knows about depression, and how science found that out. They were also a chance for researchers to find out what people with lived experience wanted to know, and what insights we have, from our different perspective.
Members also came up with questions that we wanted science to answer, discussed methods to do that and ran a small piece of research together with researchers.
How did it work?
People took part in Depression Detectives who had experienced depression, or who worked or volunteered with people experiencing depression. The project was organised via private Facebook groups which did not appear on members’ timelines.
If you want to get updates on this project or our future work, please subscribe to our mailing list below:
In this video, Sophia talks about finding out from a parent that there was almost no scientific research about something which pretty much every parent has wondered – how to deal with tantrums!
Are there questions about depression you think science should have tried to answer? We’re inviting people with lived experience of depression, or working with people with depression, to look for the gaps in mental health research, quiz researchers and design their own experiment.
If that’s you and you’d like to get involved, please go to this link to read our participant information sheet and answer a few questions about yourself. We’ll then invite you to a private Facebook group where the project is taking place.
[This project is now finished, but we will leave these posts here as a record of what we did]
We’re really excited to announce that Depression Detectives is starting today, and you can now join the group and get stuck in.
We’re looking for people who have experienced depression in the past (with or without a diagnosis) or who work or volunteer with people with depression. No research background needed! Participants will get to quiz researchers studying depression, come up with questions we want science to answer, and run a research study together with researchers.
[To take part, people read a participant information sheet and answered a few questions about themselves. We then send them the link to join a private Facebook group, which is where the project was based. Only other group members were able to see posts or who else was a member.]
We would love to have as many people involved from the beginning as possible, but new people can also join at any point during the project, so please do continue to share with anyone who might be interested.
Today we’ve got something for your ears! As part of Sophia’s previous citizen science project Parenting Science Gang, the team produced a series of three podcasts – they looked at why the project got started, the results it produced and the experiences people had participating. Today we’d like to share the second in the series, which was recorded at the Results Fair. Hannah Bestwick chatted to some of the parents and researchers who took part, about what they chose to study and the new and interesting things they found out.
You can find the other two episodes here, or under ‘Parenting Science Gang’ on your podcast app.
If you like what you hear, and think you would like to participate in a similar project looking at depression research, please join our mailing list here. We’ll be signing people up very soon, and are looking for anyone who’s experienced depression in the past, or has worked or volunteered with people with depression.
Before Parenting Science Gang, Sophia ran Nappy Science Gang, another radical citizen science project, which worked with over 600 parents who used reusable nappies on their children, and had questions they wanted to answer with science. They ranged from people with one science GCSE, to research scientists with PhDs in various areas.
This article by Andrew Maynard asks “Can citizen science empower disenfranchised communities?”. It talks about both Nappy Science Gang and a very different project, the Flint Water Study, which looked at lead levels in tap water in Flint, Michigan. Although these projects studied very different things, they shared an idea: partnering members of a community with experts to study the questions they want answered.
Depression Detectives will do the same kind of work with people who have either experienced depression in the past, or worked with people who have. If you think you might like to get involved, please join our mailing list here and we’ll let you know when the project launches and we’re signing people up.