Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
‘The Armchair Sociologist’ YouTube channel has just been launched. This is part of the Edinburgh Decameron project, and links to it are provided via the Armchair Sociology tab on the homepage. It features very informal ‘warts and all‘ conversations concerned with the process of rethinking sociological imaginations in progress. The first three videos have been uploaded and within just a day or two are already achieving a good number of views. These and the conversations to come are all concerned with how sociological imaginations of different kinds might respond to the fundamental issues that varied experiences of the coronavirus pandemic and all that goes with it are raising.
Excellent discussion of contradictory facets in UK government policy for tackling the pandemic published in the The Guardian (access here) on 12 May, by Devi Lalita Sridhar, Professor of Global Public Health, University of Edinburgh. One: track, trace, tame? Two: slow the spread, build health capacity for cycles of lockdown and release? Three: do nothing, brave new herd immunity world with UK millions dead? No, even better – a headless chicken tack between them – “It’s almost impossible to decipher which path the UK government has chosen. Over the past months, its response has vacillated from the third approach to the second and, more recently, to the first”. Important reading.
Annette Hay is an archivist and Special
Collections librarian at the Auckland Public Library in New Zealand. Mary
Holmes is a Professor in the Sociology Department at the University of
Edinburgh. In the 1970s they attended Northcote Primary School together.
The big grey concrete building was a bit intimidating,
but inside the classroom was big and lit up by huge windows. As we started
school Annette’s great aunts delighted in telling her that she would be
learning in a building that her great-grandfather had died in. Northcote
Primary School, had been used as a temporary hospital in the 1918 influenza
epidemic. That big grey building had only just been built, and as the flu hit
New Zealand that November, it was quickly put into service.
Northcote Primary School as a hospital, Auckland Libraries Heritage Collections, BO155Auckland Libraries Heritage Collections. 1571-2
There was
a lesser wave of flu that went through the country some months before the bad
one hit in late October 2018. The first wave affected the vulnerable: elderly,
babies, and those with underlying illnesses. When the second more deadly wave
arrived it killed off the healthy younger people, those in the 20 to 40 age
group. One of the theories for this was that the more vulnerable who had caught
and survived the first wave, had built up antibodies, and those who it hadn’t
touched had no defence against the second wave. In just over two months
the flu proceeded to kill around 9000 New Zealanders (the country’s population
was around 1,150,000), hitting Maori communities particularly hard. There was a
special graveyard created for Maori victims of the influenza in Northcote. It
was at Awataha, near what is now Akoranga Drive. Some dispossessed Maori lived
there in the early twentieth century, given sanctuary on land owned by the
Catholic church until they were removed in the 1920s by the church and white
settlers eager to more intensively farm and build on the land. Colonialism and
wider world events played their part in the tragedies of the epidemic.
It is impossible to separate the story of the 1918
flu and the soldiers of World War I. As the war approached its eventual end on
the 11 November, the stories of the epidemic are mixed up with the stories of
returning soldiers. Annette’s grandfather, Will Hay, was one of those soldiers.
In 1916 Will joined up and served with
the New Zealand army in France, he survived gunshot wounds, gas and influenza,
but arrived back in New Zealand at the end of 1918 to find that his father had
died of the ‘Spanish Flu’ on the 25th of November, aged 51. Scottish
born Balfour Hay had been nursed until he died in what became our primary
school class room.
The epidemic was
another blow to a country reeling from the loss of 18000 New Zealanders in WWI,
but Northcote seemed to escape relatively lightly in the flu epidemic, with only
10 deaths in the official records. Like the current Covid 19 crisis, however,
the count can be contested. For example, newly-wed Gladys Maxwell was
from Northcote but died, aged 26, nursing her husband in a military training
camp near Wellington. She was probably not counted in the Northcote toll. Nevertheless, it does seem that Northcote
did not fare so badly. Why?
Northcote is a suburb of Auckland, NZ’s largest city, and now it is only 15 minutes drive across the harbour bridge to the city centre. But in 1918 there was no harbour bridge, although regular ferries ran to the city and the population of Northcote had grown to around 1600 – hence the need for a new school building.
Perhaps Northcote’s death toll was relatively low because the narrow piece of water between it and the city helped Northcote isolate? Perhaps it was because it was a village-like and almost semi-rural suburb (known for its strawberry growing) where most people were not wealthy but lived in comfort in houses on reasonable sized plots of land? They had some distance from each other and many grew vegetables. There were not the close together houses and poverty of some of the inner city suburbs that fared much worse. Perhaps however, being able to receive care locally may have made a difference, preventing locals who fell ill from having to go to the overfull Auckland Hospital. Perhaps the care people received in our primary school classrooms was so good that most recovered?
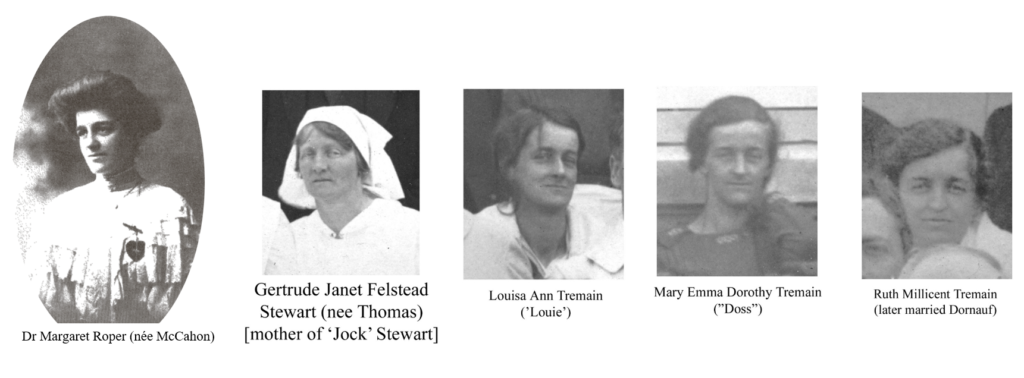
The mayor of neighbouring Birkenhead at the time was
certainly reported in the Auckland Star as
being of the opinion that without the efforts of staff at the hospital, there
would have been many more deaths in the districts. He particularly thanked the
Doctor in charge of the hospital, Dr Margaret McCahon (probably the woman in
the middle of the front row of the framed photograph above), who later married
and became Margaret Roper. Margaret, born in Timaru, in the South Island of New
Zealand, was 36 at the time and she came with experience, having been medical
inspector of schools for Otago and Southland and Medical Officer at St Helen’s
Hospital in Auckland. Margaret was in charge of nurses and volunteers,
including some of Annette’s great aunts Ruth, Doss and Louie Tremain and
Gertrude Stewart – mother of ‘Jock’ Stewart, a close friend of Mary’s uncle. As
it turns out, Margaret McCahon travelled abroad to do her medical training. She
graduated MB ChB from the University of Edinburgh in 1908.
Photos from Dovetail Archives, Annette Hay’s collection
Somehow the big grey concrete building seemed haunted but
not tainted by that epidemic. But that is just a memory. The building was
demolished in the late 1970s, just over 50 years after it was built. The layout
of separate classrooms was no longer thought appropriate for new ways of teaching.
Of course, the point is not really to remember the building, but to remember the
victims of the epidemic and the staff of nurses and volunteers who were under
the direction of Margaret McCahon.
Sources
Auckland Star, (1918) ‘The Epidemic. Return to Normal. Northcote and Birkenhead Districts’, 2 December, page 6.
Rice, G. (2005)
Black November: The 1918 influenza
pandemic in New Zealand. Christchurch: Canterbury University Press.
Verran, D. (2006) ‘The Northcote Fuel Tank Farm to1989’, Speech given to the Birkenhead Historical
Society, 13 May.
Wordsworth, J (1985) Women of
Northern Wairoa. Orewa: Jane Wordsworth, pp 51 – 54.
I write this as a settler colonial person living and working on the lands of the Gadigal people of the Eora nation that were stolen, with this theft and its related genocides never acknowledged and the land never ceded.
I’m a queer, child-free person living alone during social distancing in Sydney, with my partner a 10 hour drive away in Melbourne and my family in UK. I returned from the UK mid March and had two weeks of total home quarantine, followed by social distancing and haven’t hung out with anyone IRL for 2 months. Look, I’m doing fine. My job is stable, I can work from home, I have excellent income, I have zoom, but this vantage point allows me a particular perspective on some of the discourses I see coming out of the media at this time.
One thing that has been irking my sociology of gender brain is the repeated invocation of ‘families’ by Government spokespeople. How they are working to help Australian families. Never people, citizens, always families. They love that discourse here in Australia and we all know what it means: nuclear, heterosexual, white families. Your regular mum and dad Australians. It is this constant barrage in the media of how families can struggle through Covid, how couples can balance home schooling, how it would be preferred if you don’t visit your country / beach property (!!), how women are bearing the brunt of home schooling. And my life is so.far.from.this. And it feels sometimes that even the critical people have slipped in to an extreme reformism, a really liberal feminism where we are talking about how to acknowledge and manage that (heterosexual, parenting) women are unequally disadvantaged by lockdown and will suffer in their careers, and don’t really talk about why they are and how we could avoid it in the first place. And I’m like yes let’s be mad at how institutions don’t acknowledge the realities of heterosexual parenting women’s lives but CAN WE PLEASE BE ANGRY AT THE MEN! But more so at heterosexuality? And gender? It is this constant tension we have in politics or social change in general of dealing with and minimising the negative impacts of the world as it is (heightened in a time of crisis) and avoiding the accidental reification of the fundamentally social things that make the world how it is. It is a constant tension in my work and in feminism and gender politics. That of keeping one eye on the gender order as is and naming it (in my last book with Chris Agius we used the more 80s term masculinism to talk about it), without reifying it so we always have another eye on getting rid of it, of radically altering it. So, I wanna talk about BOTH the reality of how many of my heterosexual parenting women colleagues will be doing even more in this time, and how compulsory, state sanctioned heterosexuality causes this.
So, I leave my house and I walk down the street in my neighbourhood where I see queer couples holding hands, single people, and big extended Vietnamese families sharing houses and all hanging out in the yard or the restaurant they run (now take away, phew), to remind myself that this Australia of the news is indeed not the Australia I live in. I love my gaybourhood, one of many in one of the world’s gay capitals that I live in, I love the multiculturalism where communities keep their languages and foods and family ties, and I wish the media would stop trying to erase and deny this reality of what makes Australia awesome.
For those who can read French, here is an article by Gil Viry and Eva Nada on the lockdown published in the Swiss newspaper Le Courrier on the 5th of May 2020. They argue that the ‘stay at home’ discourse chimes with a romanticised model of the family based on the nuclear home. Yet, many people among the most vulnerable groups cannot stay safely and healthy in their homes: essential workers in precarious jobs, homeless people, women and children experiencing domestic violence, older people living alone, post-divorce families, etc. By favouring a lifestyle over others, this discourse can therefore stigmatise other cultures and lifestyles. https://lecourrier.ch/2020/05/05/un-discours-universel-stigmatisant/
This works well in Google Translate if your French is non existent like mine.
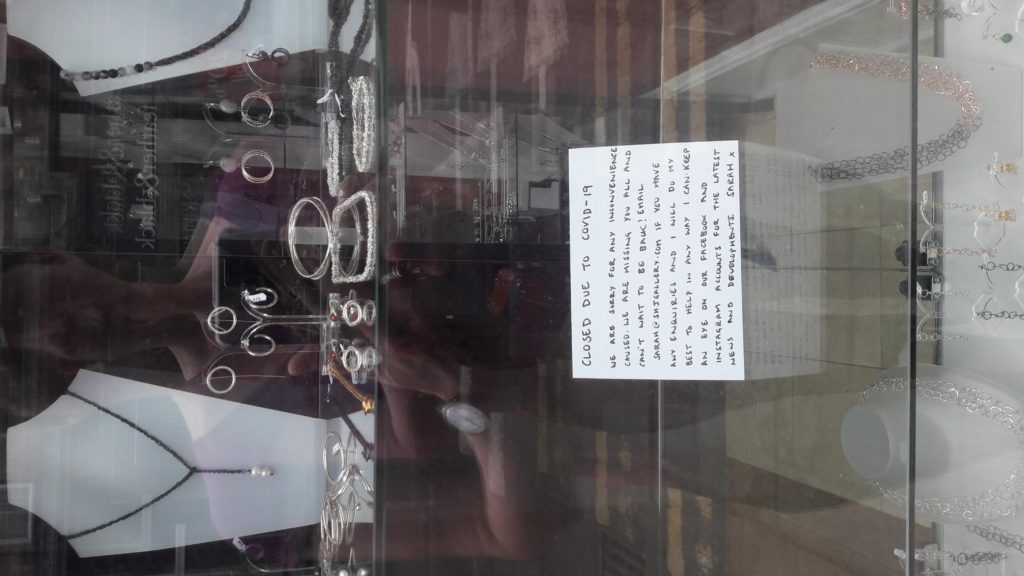
It was a beautiful morning: warm, summery. I decided to go out on my isolated walk early. This meant it was quiet and I was able to stop and take photos of some of the closed notices in the local shops. It gives just a taste of some of the small local businesses affected by Covid 19.
Katie Metzler is an associate vice president at Sage Publishing and involved with social science outputs for over for 15 years. Writing in the Times Higher Education Online, accessed here, she has posed the question of whether the coronavirus pandemic ultimately will be a good or a bad thing for the social sciences, because the social sciences can ask the kinds of questions and examine the kinds of topics that the expertise from other disciplines does not take account of. Criticisms, she points out, have complained that the government might listen to social science at all because only medical expertise is seen to really count in present circumstances. So much for Twitter and other social media and their users’ comprehension of what is currently unfolding. She also proposes that the research agendas of the social sciences will need to change profoundly, for “it does feel as though this is the time for the whole to become greater than the sum of its parts, and for specialists to bring their expertise and insight together not just to cope with the crisis but to help promote a regrowth of culture, society and economy in ways that enable future generations to further flourish”. But can and should disciplinary differences be elided in the way implied here, what about different agendas and approaches and the benefits of pursuing these rather than mashing them together? Also the idea of ‘promoting regrowth‘ seems rather tame and mechanistic, especially when the current mood seems to be more one of seizing the opportunity to make something better.
Armchair Sociology is a series of informal ‘in progress’ conversations on key challenges either brought into being or raised to consciousness because of the coronavirus pandemic and which sociological imaginations need to get to grips with. For more information, visit the post on What’s happening to sociological imaginations?. Facilitated by Liz Stanley, this conversation with Orla Murray is concerned with the ways in which sociality and relationship are being remade, including in relation to teaching and researching, as we enter a ‘social bubble’ context.
Dr. Órla Meadhbh Murray is a feminist sociologist who completed her PhD in Sociology at the University of Edinburgh (2018). Her PhD used Dorothy Smith’s work on institutional ethnography to explore UK university audit processes. Órla is currently working at Imperial College London on SIDUS, alongside developing methodological resources and writing a monograph based on her PhD (forthcoming 2022, Bristol University Press).
Armchair Sociology is a series of informal ‘in progress’ conversations on key challenges either brought into being or raised to consciousness because of the coronavirus pandemic and which sociological imaginations need to get to grips with. The conversations are facilitated by Liz Stanley, with the first with Jennifer Morris and Derek Morris on time and the oddities of how it is being experienced under lockdown ‘social bubble’ circumstances by differently situated people.
This first conversation was something of a try-out, not so much of the topic, as we had email exchanged about this previously, but how best to record it. Skype was the preference because likely to be on people’s machines in different parts of the world, and Zoom and Teams among others less so. But there were some problems with two people sharing one laptop not visible when recording – in going for the midpoint, the software cut off bits of Jen and Derek in playback. We did it again – but the spontaneity and fun went. So we present here something technically flawed, but really enjoyable to have been part of. And we’ll know better next time.
The recording we made can be accessed on YouTube here.
Derek Morris is a PhD student in Socio-cultural Studies at the University of Edinburgh. He is a US Iraq War veteran with research interests in soldiers and their relation to society through autoethnography, narrative inquiry, and the Documents of Life approach. He has worked as a research assistant in GIS on a NASA Space Grant, taught ESL in Istanbul, Turkey, and received an MPhil in Race, Ethnicity, Conflict at Trinity College, Dublin.
Jennifer Morris is a freelance writer, designer, and editor in online language exam development. She is a founding member of the Communicative English Proficiency Assessment (CEPA®) and its associated research and development group in Turkey, though she lives with her partner who is a PhD candidate in Edinburgh. She is in the final phase of publishing a study in her field on the praxis of Evidence Centered Design (ECD) framework. She holds a MA in Applied Linguistics from the University of Massachusetts and her research interests include foreign language pedagogy and testing development, language policy, sociolinguistics, and institutes of higher education.
The
viral character of how some
media stories circulate – with a current story picked up by other media
sources and
multiply repeated
with minimal changes or by transferring it into local examples – is well known. Thus Llandudno goats coming down from the hills to roam the town streets fetches up with a
media story in Brazil and
sheep in one of its cities. And similarly with key terms and ideas which
circulate and recirculate: for example, there has been a flood of reporting
that lockdown is restriction and a liberties infringement and the suffering it
engenders (all that sitting on sofas eating snacks and watching TV) is treated
as on a parallel with being bombed in the Blitz. And at a point when hospital
deaths might be declining though still high but those in care homes certainly
aren’t, comes many journalists over the last few days reporting, promoting,
encouraging, anticipating, the lifting of lockdown and the need for exit strategies.
Little else is being reported – it‘s coronavirus coronavirus
coronavirus – and trying to find new angles on this to fettle up for today‘s
reports. Into the mixture comes ‘the experts’, and hunt the tame expert by journalists who seize upon a statistician here, an epidemiologist there, a frontline doctor there, a
cancer specialist here, a chief medical officer there. The obsession in the
first 10 days of May has been with lifting the lockdown, the exit strategy, the
five rules for lift up and other buzz terms currently in circulation. From the
start and even before the term pandemic was used, there have been ideas about
more rigorous distancing rules for groups of people characterised as
particularly vulnerable. In the present rush in the world of media journalists
to lift lockdown, these have been joined a few days ago by another such buzz
term, ‘segmented shielding’.
While well meant, initially at least, ideas about
vulnerability and shielding have important negative consequences for
independence, autonomy and agency, for personhood. On the one hand there are GP
practices in the UK that have issued letters asking ‘vulnerable’ people – those
over 70, and those with disabilities in specialist care homes – to sign forms
agreeing to not being resuscitated, while on the other hand there is ‘extend
the lockdown’ for some groups being advanced. Interestingly, the idea of ‘herd immunity’ heard much at an earlier point lies
at back of the ‘segmented shielding’ idea just reported in the news
media.
On 7 May, a number of news reports appeared in the UK concerned
with this idea of segmented shielding. “The Coronavirus: Is it time to
free the healthy from restrictions?” item on the BBC news app by a ‘Health
correspondent’, for example, gave it prominence by reporting on a piece of
epidemiological modelling with quoted comments from its lead researcher. It
also repeated such phrases as ‘experts have
found..‘ and ‘researchers have shown’, various of which appear in a press
release from the research team (which can be accessed here).
The BBC news item is structured using quotations from a number of
designated experts stitched together with an ‘it is so’ kind of narrative
commentary. Younger people are said to be less at risk than they think,
and those who died or had severe coronavirus most likely had unrealised
underlying health factors – “…we have “lost sight” of the fact the
virus causes a mild to moderate illness for many, says Dr Amitava Banerjee, of
University College London”. It continues, it is also important to take full
account of other costs, emotively including domestic violence, mental health
problems and restricted access to other healthcare, leading to the implicit
weighing of these against the cost of further deaths, which from the commentary
and linked graphs are largely those of the elderly and vulnerable.
Segmented shielding enters frame here via comment about an
Edinburgh-London research project, to the effect that restrictions could be
lifted if the most vulnerable are shielded. This is backed by a quotation from
the team leader that for most people coronavirus carries no more risk than a
“nasty flu”. Researchers from Stanford University are then brought
into play, in calculating
the UK risks for those under 65 as equivalent to driving 185 miles a day, “with
deaths in non-vulnerable groups being “remarkably uncommon”.”
The BBC news report seems remarkably okay with the idea of
dividing the population and imposing strict restrictions on everyone designated
as vulnerable. It also accepts without question calculations as to the proposed
minimal impact of coronavirus on the rest of the population, seeing its members
as largely herd immune or only minimally affected. However, there is more
to the idea of segmented shielding than appears in the news report, found in
the research press release and associated full report (which can be accessed
from the press release referenced above).
The Edinburgh-London press release writes of its own work in terms
of expertise and in a third-person voice – “experts suggest, researchers say,
academics from the Universities of Edinburgh and London, researchers say, the
team proposes, the team says, the team stresses”. It is in fact
recipient-designed as a press release produced with journalist-use in
mind. The result is that its claims can be inserted into ‘news reports’ as
though the reporter is designating the people concerned as experts, rather than
this being a self-designation. The press
release contains a link to the research paper reporting
the piece of mathematical modelling carried out. The typescript report writes
that:
“Key risk factors for vulnerability to COVID-19 are defined by the World Health Organisation (WHO) as those over 60 years old and those with underlying medical conditions (such as cardiovascular disease, hypertension, diabetes, chronic respiratory disease, and cancer)…
We enumerated these categories using published data… For our baseline scenario we designated 20% of the total population as vulnerable. We assumed a 1:1 ratio of shielders to vulnerable. The remaining 60% of the population are not in either category and we refer to this as the 20-20-60 model…”
Problems with this are clear. The calculation of risk factors for those deemed not vulnerable have to be accepted as 100% precise, assumptions about how coronavirus infections spread have to be watertight, certainty in identifying vulnerability has to be absolute, and the one-to-one ratio of ‘shielders to vulnerable’ has to be fully accurate. The untenable character of calculations of risk, assumptions about infection spreading, and identification of underlying health factors, are sufficiently obvious as not to require elaboration here. The shielder/vulnerable ratio is also dubious, for those with the most serious health issues require significantly more assistance than from one person. But even supposing all these were not disputed claims but factual certainties, how to achieve an impermeable separation between the herd 60%, the shielder 20%, and the vulnerable 20%?
“…Measures including self-isolation of cases, quarantining of affected households, contact tracing and voluntary physical distancing will be necessary to achieve this. In all our scenarios the vulnerable segment is subject to increased protection indefinitely…
…In addition, S&S could be greatly strengthened by infrastructure and technological support for effective biosecurity, both at institutional (e.g. care homes, hospitals) and household levels in order to keep transmission rates low between and within shielders and vulnerable populations. For maximum effectiveness biosecurity requires training, high standards of hygiene, effective personal protective equipment and screening of everyone in contact with the vulnerable population…”
Segmented shielding, S&S, is being envisaged as an indefinite
system involving biometrically-based surveillance of the vulnerable and
shielder populations, coupled with
frequent, indeed daily, medical tests to ensure compliance. The result would be a brave new world indeed, of a permanently sequestered 20% vulnerable population, a permanently routinely tested 20%
shielder population, and
an unrestricted 60% supposedly immune or resistant population. So much for
notions of independence and autonomy, and instead a state of high surveillance,
ongoing biometric and medical interventions, and indefinite sequestration for a
huge proportion of the population. Agency for the vulnerable 20% would go to
the wall for an indefinite period; and the shielder 20% would be under
indefinite multiple surveillance and have minimal agency themselves.
In the meantime, polls suggest that the majority of the UK population are not clamouring of the lift of lockdown, are not demanding for restrictions to be lifted on a privileged supposedly largely immune group. So where have these ideas come from? Is it a case of hunt the other experts, and hunt the other journalists in search of an easy story they can sex up? The buzz terms circulating provide a route into exploring this. For instance, a PS to this discussion is that on 11 May in commentary on a speech by the UK prime minister Boris Johnson, claims about most of the population being immune or only minimally affected were repeated and associated with the Edinburgh and London research as well as the same Stanford and Cambridge comments. The strong indications are that once in circulation there is a high chance of such buzz terms and ideas being recirculated and recirculated.
The alternative to the ‘brave new world’ of the herd and the vulnerable and its appalling prospect is not to do nothing, but to look for non-discriminatory ways forward that do not have the implied eugenicist basis of this. Eugenicism has already raised its ugly head in the rash of GP practices issuing letters and forms about non-resuscitation; segmented shielding and biometric interventions are another variant. And the alternatives? Vaccines and related treatments along the lines of managing HIV/AIDS, and mass changes in expected behaviour in which everyone observes a social bubble approach, are among them.