Any views expressed within media held on this service are those of the contributors, should not be taken as approved or endorsed by the University, and do not necessarily reflect the views of the University in respect of any particular issue.
If you’ve noticed that my blog thumbnail is just a small red square, that’s not an accident.
It’s actually the NATO maritime signal flag for Foxtrot (F).
In the International Code of Signals, every single flag has a specific meaning when flown on its own. For example:
The Alpha (A) flag means:
“I have a diver down; keep well clear at slow speed.”
It’s a way of communicating vital information quickly and clearly, across language barriers.
So what does Foxtrot mean?
“I am disabled; communicate with me.”
And honestly, that fits this blog about as perfectly as anything could.
At the heart of disability and autism advocacy is a simple principle:
Nothing about us without us.
We don’t want decisions made over us.
We don’t want policies designed for us without our input.
We don’t want to be “managed”, “handled”, or quietly sidelined.
We want communication.
We want partnership.
We want to be part of the conversation.
That’s exactly what Foxtrot signals:
“I’m here. I have needs. Talk to me.”
It’s also a little nod to the fact that I love sailing, and that maritime signalling systems are, in many ways, a brilliant example of inclusive design: clear, standardised, visual, and accessible across cultures and abilities.
The University has over 200 of policies. (All here)
They overlap, cross-reference each other, and are written for different audiences.
That is overwhelming, and very few people — disabled or not — read them all.
This guide is here to:
point you to the few policies that actually matter most for disabled staff,
explain why they matter,
and help you understand what to do in practice, without expecting you to become an HR or legal expert.
The one policy every disabled staff member should read
Reasonable Adjustments Policy
If you only read one policy, make it this one. (Link)
This policy sets out:
your right to reasonable adjustments at work,
the University’s legal duties under equality law,
how adjustments should be requested, considered, and implemented.
Reasonable adjustments can include (but are not limited to):
changes to hours, workload, or deadlines
flexibility in location or working pattern
physical or digital accessibility changes
support with communication, meetings, or assessment processes
📌 Important:
You do not have to be “visibly disabled”, formally registered, or struggling badly before asking.
Adjustments are about enabling you to do your job on an equal footing, not about proving hardship.
Policies that are especially relevant for disabled staff
You don’t need to read all of these right now — but it is useful to know they exist.
Absence Management Policy
Read here. Disabled staff are statistically more likely to:
have fluctuating health,
need time off for treatment,
experience periods of higher absence.
This policy explains:
how sickness absence is recorded,
what happens at review points,
how disability-related absence should be considered differently.
📌 Why this matters:
If absence becomes an issue, this policy interacts closely with reasonable adjustments.
Knowing this exists helps you advocate early, rather than only once problems arise.
Capability (Performance Management) Policy
The University also has a Capability Policy (sometimes referred to as performance management). Read here.
Disabled staff are statistically more likely to be drawn into capability processes, particularly where:
health fluctuates,
fatigue, pain, or cognitive load affect output,
or reasonable adjustments have not yet been put in place.
This policy explains how the University manages concerns about performance.
📌 Important:
If you are disabled, reasonable adjustments must be considered and put in place first where performance concerns may be linked to disability.
Adjustments should:
be agreed,
be implemented properly,
and be given time to work.
As a rule of thumb, adjustments should normally be in place for around three months before capability or performance management is considered, so it is possible to see whether they resolve the issue.
If capability is raised before adjustments are in place, or without allowing time for them to have an effect, that is a red flag.
If performance concerns arise and you are disabled, you can:
ask whether reasonable adjustments have been considered,
contact the Disability Officer for support,
or seek advice from HR or your trade union.
📌 Key point:
Capability processes should not be used as a substitute for putting reasonable adjustments in place. Knowing this policy exists helps you challenge that early, rather than once a formal process has started.
📌 Why:
If a building, system, or piece of digital content is inaccessible:
that isn’t just “unfortunate”,
it may be a policy breach.
That gives you:
stronger footing when raising issues,
clearer routes for challenge,
and language that moves the conversation from “personal problem” to “institutional responsibility”.
Menopause Policy
The University also has a Menopause Policy. Read here.
Menopause and perimenopause can affect people in very different ways.
Symptoms can be:
physical,
cognitive,
psychological,
and may fluctuate over time.
For some people, this can have a significant impact on work, including attendance, concentration, memory, temperature regulation, sleep, and energy levels. Therefore it falls under the widest interpretation of the Disability Umbrella.
This policy sets out that:
support is available,
reasonable adjustments can be put in place,
and menopause is treated in the same way as other long-term or fluctuating health conditions.
📌 Key point:
You do not have to “push through”, minimise your symptoms, or wait until things become unmanageable before asking for support. The policy exists to support you, not as a last resort.
A reality check (and some reassurance)
The University is trying to be inclusive.
The policies are there, and in the right spirit. Implementation lags behind, not due to malice but due to systemic issues.
But:
implementation is uneven,
knowledge varies wildly between managers,
and disabled staff often end up doing extra labour just to make things work.
📌 The important bit:
You have rights, and you have policies you can point to.
That matters — even when progress feels slow.
What to do if you need adjustments
If you know what you need
Talk to your line manager
Ask for reasonable adjustments.Best case, that’s all you need.
If adjustments are agreed, they should be implemented and reviewed, not treated as a one-off favour.
If adjustments aren’t happening, or you’re not sure what you need
Contact the Disability Officer. Website and email.
Their role is to:
help you identify appropriate adjustments,
support discussions with managers,
and reduce the burden on you to “get it right first time”.
This is a normal, supported route — not an escalation.
Occupational Health while OccHealth can assist with adjustments for medical conditions, they are very rarely your first point of call unless you return from long sickness leave. We would recommend reaching out to the Staff Disability Advice Service first.
You’re not doing this alone!
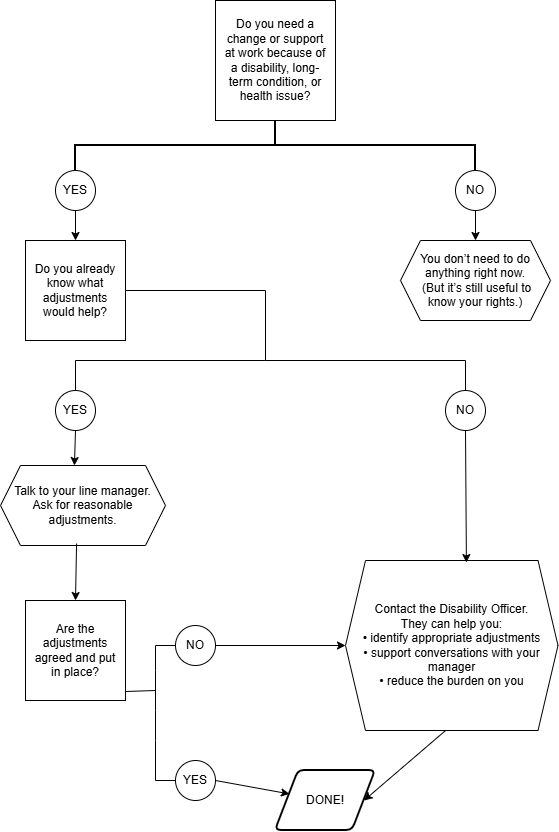
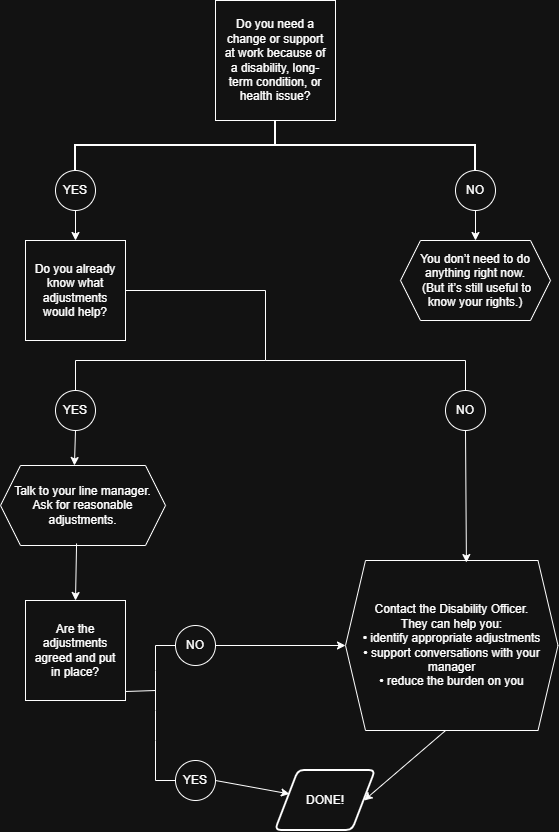
Flowchart: What to do
Text version of the flowchart
Start.
Ask yourself:
Do you need a change or support at work because of a disability, long-term condition, or health issue?
If the answer is no:
You do not need to do anything right now.
It is still useful to be aware of your rights in case your situation changes in the future.
If the answer is yes:
Ask yourself the next question.
Do you already know what adjustments would help?
If the answer is yes:
Talk to your line manager and ask for reasonable adjustments.
Next, consider:
Are the adjustments agreed and put in place?
If the answer is yes:
No further action is needed at this time.
Review the adjustments later if your needs change.
If the answer is no:
Contact the Disability Officer for support and guidance.
If you did not know what adjustments would help:
Contact the Disability Officer.
The Disability Officer can help you to:
identify appropriate adjustments,
support conversations with your manager, and
reduce the burden on you to work out solutions on your own.
Final outcome:
Adjustments are discussed and agreed, with support if needed.
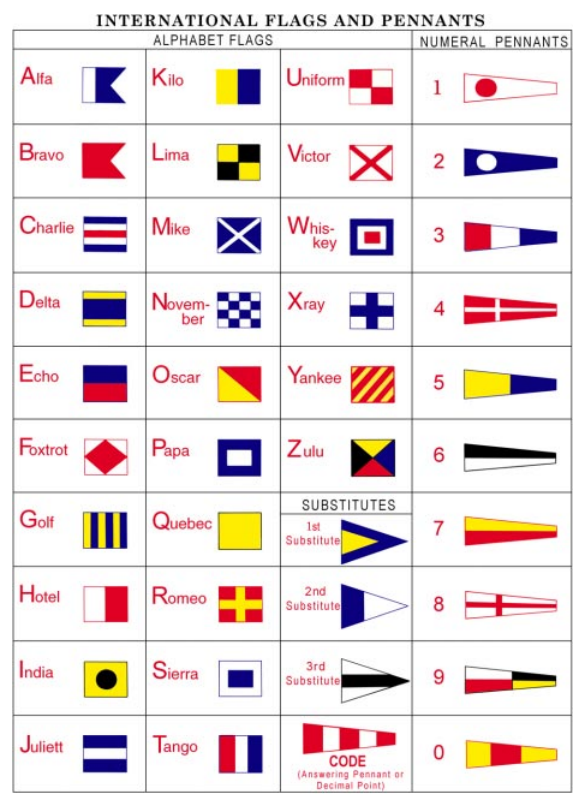
Today in “things that are inclusive and you didn’t realise they are”:
the International Code of Signals (ICS)
From the INTERNATIONAL CODE OF SIGNALS UNITED STATES EDITION 1969 Edition (Revised 2003)
We tend to think of inclusion as something modern — a recent design concern introduced in the last decade or two. But hidden throughout history are whole systems that ended up being quietly, unintentionally inclusive because they had to work for everyone, under every condition.
One of the best examples? The International Code of Signals (ICS).
What is the ICS?
The International Code of Signals is a global communication system used by ships at sea. Long before radios were reliable, vessels relied on flags, lights, shapes, and sound signals to communicate essential information between ships, between ship and shore, or during emergencies.
The modern ICS alphabet was standardised in the mid-19th century, gradually refined by the British Board of Trade, and formally internationalised in the 20th century. The point was simple: every ship in the world, regardless of language, must be able to understand the same messages.
How the system works
The ICS includes:
26 alphabetical flags (A–Z)
10 numeral pennants (0–9)
3 repeaters (1st, 2nd, 3rd) to repeat letters in hoists
Special flags for code groups and signalling conditions
Each flag has a distinctive combination of shapes, stripes, blocks, and layout. Crucially: each flag also carries a meaning beyond its letter.
Examples include:
A – Alfa: “I have a diver down; keep well clear.”
B – Bravo: “I am carrying dangerous cargo.”
O – Oscar: “Man overboard.”
V – Victor: “I require assistance.”
It is an entire international language, designed to cut through uncertainty, weather, and linguistic barriers.
Victor means “I require assistance.” or ” Ich benötige Hilfe” or “Je demande assistance.” or “Ég þarfnast aðstoðar.”…you get the idea.
In an emergency even an old times sailor (who historically often couldn’t write or read, as opposed to officers) could raise a “I require medical assistance.” flag (Whiskey) with know how to spell any of that.
So where does inclusion come in?
The ICS had to work:
In fog
In storm conditions
When flags faded in the sun
From long distances
On ships crewed by people from all over the world
And crucially: without relying solely on colour
This last point is where the hidden accessibility appears.
Historically, navies and merchant fleets were overwhelmingly male environments — and roughly 8% of men have some form of colour-blindness. For most of history, there was no colour-vision testing for sailors. You simply took whoever could work a deck, haul a line, or man a watch. (Or in the earlier days of the Royal Navy, any drunk bastard who could make three xxx on a piece of paper and was too drunk to run away…)
If the flag system had depended on exact colour discrimination, it would have failed immediately in real-world use.
So the system was designed to be recognised through pattern, geometry, and contrast, not colour alone.
Why ICS is inherently colour-blind inclusive
Even though the flags are coloured, what actually makes them identifiable is:
Horizontal vs. vertical stripes
Diagonal bars
Chequered patterns
Centre squares or blocks
Unique proportions
Strong dark–light contrast (important in greyscale vision)
Shapes that still read correctly when bleached by sun or salt
This means a sailor with red–green colour-blindness (by far the most common) can distinguish “Oscar” from “Zulu”, or “Bravo” from “Hotel”, from the pattern alone.
The ICS is, unintentionally, a great example of pre-modern universal design.
It is inclusion by necessity — because you cannot run a global system that depends on perfect colour perception, perfect weather, or perfect conditions.
A lesson from maritime history
The ICS shows something important:
When a system is designed to succeed under pressure, uncertainty, and real-world conditions, it often ends up being more inclusive.
Accessibility isn’t always a modern invention. Sometimes, it’s baked into the oldest tools we have — quietly doing its job, unnoticed, because it had to serve everyone long before inclusion became a buzzword.
Hidden inclusion really is everywhere.
Everyone Wins
That’s the heart of it: inclusive design never creates a burden — it creates clarity.
Even with perfect colour vision, I find it far easier to read what the ship in front of me wants because the system was built to work for everyone. Inclusion doesn’t make things easier for disabled people and harder for everyone else; inclusion makes things easier, safer, and more reliable for all of us.
Universal Design and Individual Tailoring: Why We Need Both
People often frame accessibility as a choice: do we build universally, or do we tailor individually? The reality is—of course—we need both.
Universal Design: dignity, efficiency, and reduced labour of inclusion.
Universal Design (UD) is often sold as a magic solution that will “catch everyone.” It won’t. It never will. And that’s fine, because UD isn’t about perfection—it’s about coverage.
When we design materials, systems, spaces, and processes so they work for as many people as possible, several good things happen:
Fewer people have to declare their disability, which protects dignity and reduces the emotional admin of constantly explaining your needs, it reduces Labour of Inclusion.
Time and money are freed up to support the people who do require tailored adjustments.
Workload becomes manageable, because you’re not reinventing the wheel for every individual request.
A simple teaching example:
I have 120 students in a lecture. Out of them:
10 are dyslexic
1 has visual issues (I don’t use impairment anymore, the Blind community feels strongly about this!)
1 needs large print
If I make inaccessible slides (e.g., Times New Roman, poor contrast, cluttered layout), I now have to respond to 12 individual adjustment schedules and produce multiple versions.
That is not a good use of my labour or institutional resources.
If I instead make one fully accessible slide deck from the start—clear font, high contrast, good structure— I immediately meet the needs of 11 students. Now there is only one student who requires a tailored version, and I actually have time and energy to give them what they need.
UD actually is a resource management tool.
Universal Design is not universal
There’s a myth that UD, if done well enough, will cover everybody. It won’t. Human variation is vast and always will be.
UD doesn’t replace individual adjustments. UD creates capacity for individual adjustments.
Think of it like triage in reverse: cover the majority up front, so you can do justice to the minority who require something different.
That is what real equity looks like.
Why both approaches matter
UD preserves dignity by removing the need for constant declarations. Tailoring preserves equity by responding meaningfully to those whom UD cannot help.
Both matter.
And both are required.
But we also need systems to support this balance—for example:
Digital adjustment records that follow a person across departments or institutions
Reduction of repetitive disclosure
Consistent accessible design standards
The point is simple: Universal Design is not a replacement for individual adjustment. It is the foundation that makes genuine equity possible—by freeing up resources to respond well, respectfully, and promptly to those whose needs fall outside the majority design.
Dual approaches aren’t a compromise. They’re the only way forward.
Work Package One, part of WhoCares, starts with the most fundamental question in disability governance:
How does policy need to be designed, structured, and embedded so that it actually works for disabled staff — not just on paper, but in everyday practice?
Universities often assume that writing a good disability or reasonable-adjustments policy is enough. WP1 shows why this isn’t true. A policy is only one component in a much larger system of recruitment, onboarding, HR procedures, line management, IT access, estates, health & safety, culture, and communication. If any part of that system fails, the policy fails with it.
What WP1 Does
WP1 maps this whole system — the “policy machine” — using approaches borrowed from systems engineering, aviation safety, and human factors. It looks at:
The policy itself: clarity, structure, responsibilities.
The policy network: how related policies reinforce or contradict it.
Implementation chains: who needs to know the policy and who actually does.
Human factors: workload, communication breakdowns, unconscious bias, norms, and the predictable ways people misinterpret, forget, or avoid policy.
The labour of inclusion: the hidden work disabled staff do because the system hasn’t been designed around them.
The aim is to diagnose where disability policy collapses: not at the level of legal compliance, but at the point of lived experience.
Why This Matters
Disabled staff do not experience “a disability policy.” They experience the entire ecosystem around it.
A policy will only work if:
it is known,
it is understood,
it fits coherently into the wider policy environment,
it can be implemented by staff with the time, training, and resources to do so,
it accounts for human fallibility,
and it does not rely on disabled staff to constantly self-advocate, educate, chase, or correct the system.
Most UK universities currently fail at several of these points, creating a wide implementation gap: the difference between what the policy promises and what disabled staff actually experience. WP1 analyses why that gap exists — and how to close it.
What WP1 Contributes
1. A systems-based blueprint for policy that works.
Policies must be written and embedded like engineering systems: with defined subcomponents, interdependent parts, and checks that each part is installed and functional.
2. Human-factors insight into implementation failure.
Policy collapses not because people are malicious, but because they are overloaded, undertrained, distracted, or following local norms. WP1 uses human-factors models (including aviation’s Dirty Dozen) to analyse these predictable failure points.
3. Practical strategies to reduce the labour of inclusion.
WP1 identifies how policies must be designed to shift the workload off disabled staff — through better communication, automatic prompts, universal design, resource allocation, and built-in accountability.
In Summary
Work Package One provides the evidence base for building disability policy that actually works. Not symbolic. Not aspirational. Operational.
It shows that effective disability policy isn’t one document — it is a functioning system, explicitly designed to overcome human factors and implementation gaps. And when that system works, disabled staff don’t just get support: they get equity, dignity, and the chance to do their work without carrying the extra labour that the system should carry for them.
For decades, the social model of disability has been one of the most transformative frameworks in disability rights. It offered a radical, empowering shift: people are disabled not by their bodies, but by barriers created by society. Stairs disable wheelchair users, not paralysis. Small print disables visually-impaired readers, not impaired vision. The problem lies not in the person, but in the environment.
This was a necessary and powerful counter to the medical model, which treated disability as an individual defect to be cured, controlled, or pathologised. The social model exposed the injustice of designing a world around a narrow idea of the “normal” body. It said: we can build something better. And it changed law, activism, and everyday access in ways that can’t be overstated.
But that doesn’t mean the social model is complete.
Where the Social Model Hits Its Limits
The social model works brilliantly when barriers are environmental or attitudinal. But it struggles — really struggles — in scenarios where pain, fatigue, neurological overload, or deterioration are intrinsic to a person’s condition, not results of external barriers.
Someone with:
chronic nerve pain
ME/CFS
sickle-cell disease
inflammatory conditions
degenerative disorders
complex neurological conditions
or severe migraines
…doesn’t stop suffering just because a ramp exists, or a workplace is accessible. No manager, however inclusive, can magically remove a pain flare or a seizure cluster. And the classical social-model line of “the disability is only in the environment” can begin to feel gaslighting for people whose daily experience is hardship.
This leads to two significant limitations:
1. It assumes suffering is always externally imposed.
This erases the lived reality of people whose bodies do cause real pain, unpredictability, or limitations.
2. It overburdens disabled people with the job of “advocating for access”.
Under the classic social model, if barriers disable you, you must identify them, explain them, request adjustments, negotiate them, and sometimes fight for them. The result: the hidden labour of navigating disability remains on the disabled person.
This hidden labour includes:
managing symptoms
managing energy
coordinating care
managing medication logistics
constantly self-advocating
endlessly explaining
covering for inaccessible systems
translating policy into reality
The social model removed some burdens, but it left too many where they were.
We need something better — something that acknowledges bodies as real, and societies as responsible. We need Social Model 2.0.
What Social Model 2.0 Looks Like
Social Model 2.0 keeps the best of the original — the focus on removing barriers — but adds a crucial layer of collective responsibility. It recognises two truths simultaneously:
Some suffering comes from disabling barriers.
Some suffering comes from the condition itself — and society must still help carry that load.
In Social Model 2.0, inclusion means more than ramps, captions, and flexible work. It means society intentionally takes on the labour that disability otherwise forces onto the individual.
Instead of saying:
“Tell us what you need, and we’ll see what we can do.”
Social Model 2.0 says:
“We assume you carry invisible labour. We proactively share that workload, because pain and symptoms aren’t a personal failing — they’re a collective responsibility.”
This model recognises that access is not just the built environment; access is the entire ecosystem of living with a condition.
What this looks like in practice:
1. Collective responsibility for accessibility basics
This part is classic social model:
ramps
clear signage
lighting
flexible deadlines
hybrid meetings
quiet rooms
sensory-friendly events
non-hostile HR processes
inclusive policymaking
accessible digital systems
But unlike the original model, Social Model 2.0 treats these not as optional extras but as organisational duties — automatically deployed, not dependent on disabled people asking for them.
2. Collective responsibility for health-related labour
This is the new layer. It says: even when a condition’s pain or instability is intrinsic, society has a duty to help.
Examples:
Ensuring someone with a painful condition has secure, reliable access to medication
Giving extra recovery time without guilt or performance penalties
Creating predictable routines so symptom management becomes easier
Making sure someone doesn’t have to fight insurance, HR, or scheduling while in pain
Assigning support workers or admin assistance to reduce cognitive and logistical load
Designing systems where disabled people are not required to “prove” their condition repeatedly
Building organisational cultures where illness and pain are assumed, not doubted
Proactively checking that people in flare or decline have their practical needs covered
In other words:
We stop pretending that inclusion ends at “remove the barrier”
and start recognising that many barriers are internal to the body — and still not the disabled person’s burden to carry alone.
Why Social Model 2.0 Matters
Because the world has changed. Because we understand more about chronic illness, neurodiversity, pain science, fatigue, and fluctuating conditions than we did in the 1980s. Because “inclusion” can no longer stop at architecture and attitudes.
And because we now know that:
Pain is real.
Fatigue is real.
Overload is real.
Recovery time is real.
Admin is labour.
Self-advocacy is labour.
Navigating inaccessible systems is labour.
Managing medication is labour.
And all of this is work disabled people are doing every single day that nobody sees.
Social Model 2.0 says: If society disables us, society must fix it. If the body disables us, society must help carry that weight too.
It isn’t about pity. It isn’t about protection. It’s about justice, dignity, and shared responsibility.
Conclusion: A Model That Finally Fits Reality
The original social model liberated us from a worldview that blamed disabled people for existing. But like any model, it reflects the era it was born in. Today, we face different challenges: long-term conditions, fluctuating illnesses, invisible disabilities, complex pain conditions, and the enormous hidden labour that comes with them.
Social Model 2.0 is not a replacement — it’s an upgrade. It keeps the political strength of the original while updating it for the world disabled people actually live in.
Because inclusion isn’t just removing barriers. It’s removing burdens.
Because disability isn’t just a policy problem. It’s a shared societal responsibility.
And because no one should have to carry their pain — or their access needs — alone.
“Autistic people struggle with language. They don’t understand when you say the horse has bolted.”
No. It’s a bit different from this.
(Also, at least say the horse has sailed, make it interesting)
What Autistic people and people who don’t speak your English struggle with is hidden meaning. Like in this post.
What do you mean “your English”, Claire? There is only one English.
*Linguist mode activated*
There are hundreds of thousands of Englishes.
Regional variation.
Class variation.
Education.
Neurotype.
Age.
Gender.
Health.
Oh, and that is just the native speakers.
And, did I mention everyone has more than one English?
You don’t speak to your granny like to the lads in the pub. Hopefully…
Okay, now where does your autistic colleague or student struggle?
Hidden meaning you can’t look up.
Let’s take email sign offs…
Kind regards: My default setting. Like a Roomba with manners. I did not put effort in. Not really kind. Regards: I’m very cross with you. Warm regards: Something is afoot. You will discover it in Act III. Best regards: I want something. I likely don’t know you and I’m just hoping for the best. With regards: I don’t speak English well and Google suggested this. Best: The salted crisp of sign-offs. Acceptable. Emotionally vacant. Thanks: I’m polite, but make no mistake — the clock is ticking. Thanks again: Please read the subtext before things escalate. My patience is now as thin as a UK bin bag. Thanks in advance: Emotional extortion in professional font. You are now forced to do what I asked for. All the best: I’m about to retire or I think you are/should be. Appreciate it: I absolutely do not. In fact, I’m annoyed you didn’t already do this. Yours truly: Romantic. Does not belong here.
Now, “regards” does not always “I’m angry with you”, it means that depending on who said it. And if you don’t know the person you have to learn to guess correctly from their role, age, skin colour, name, and the rest of the email.
That’s a lot of work and really complicated and requires a strong theory of mind (thinking yourself into someone else’s shoes).
Now what?
So, if my student/colleague doesn’t get my hint they are autistic?
Maybe. Or not a native speaker. Or from a different English speaking part where things are phrased differently. Or not that gifted with social antennae.
But, good news! You don’t have to know. Just use these 3 tips on everyone and you’re sorted:
1. No hints!
⛔ “Maybe Bauer 2012 is worth a look…”
✅ “Read Bauer 2012 please.”
2. Clear language
⛔ “This is quite good, you might want to do a little editing…”
✅ “This has potential but it is not there, yet. You will have to make substantive edits.”
3. Assume no malice:
⛔ “Bob was rude to me, I have HR on speed dial!!!”
✅ “Okay, what Bob said sounded a bit rude to me. What is the best possible interpretation of what he just said? It’ll roll with that until proven otherwise.”
Today in understanding neurodiversity: Auditory Processing Disorders
My approach: chaotic.
APDs are all about processing not sensory input. So many of us are quite good at low processing comms like radio, calling dispatch, underground radio etc. And bad at other audio only setups.
Because I am, like many people with APD, also blessed with hypersensitive hearing, I’m actually better at radios in wind and background noise than most.
Why is that an important distinction? I’m not Deaf but I have to lipread when conditions are bad. And I can still turn around and operate the radio well. That’s not mutually exclusive.
“But why can you operate a radio then, Claire? Shouldn’t you be worse at that than most people?”
Funny you ask…
Radio is easy. Why?
It follows a very simple system.
The number of things that can be said are predictable.
People speak clearly and don’t mumble.
The turn taking is verbal and explicit (“over”).
Backchannelling is verbal and explicit (“copy”).
Asking for clarification is considered good form.
There is no social bonding aspect.
There is a very strong emphasis on maximum distinction (“niner” for 9).
It’s short.